Physiology of deglutition
•Download as PPTX, PDF•
34 likes•13,590 views

DEGLUTITION (SWALLOWING)

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Physiology of deglutition
Similar to Physiology of deglutition (20)
More from Dr. Pruthvi Raj S
Recently uploaded
Recently uploaded (20)
Physiology of deglutition
- 1. PHYSIOLOGY OF DEGLUTITION Dr.PRUTHVI RAJ.S Junior resident ENT-HNS
- 2. INTRODUCTION • Swallowing involves the passage of a bolus of food or liquid from the oral cavity to the stomach via the pharynx and oesophagus, passing over the entrance to the laryngeal vestibule. • Partly reflex ; partly under voluntary control. • Co-ordinated movements.
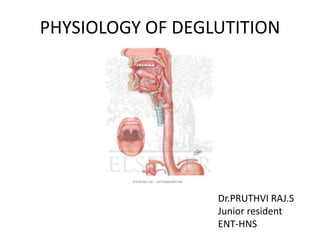
- 4. A mid-sagittal section of the head and neck showing the location of the major structures involved in swallowing. A. Hard palate B. Soft palate C. Nasopharynx D. Pharyngeal isthmus E. Oropharynx F. Laryngopharynx G. Cricoid cartilage H. Thyroid cartilage I. Hyoid bone J. Laryngeal inlet.
- 5. EVENTS ORAL STAGE Voluntary control PREPARATORY TRANSPORT PHARYNGEAL STAGE Reflex activity SWALLOWING OESOPHAGEAL STAGE Involuntary
- 6. ORAL PHASE • PREPARATORY PHASE : Jaw - closed by the jaw elevators, temporalis, masseter and medial pterygoid. Chewing - combination of elevators and depressors of mandible. Lips maintain a tight seal under the action of the orbicularis oris . Buccinator is used to return food from the vestibule during the process of mastication. Soft palate is lowered under the action of the palatoglossus and palatopharyngeus which approximate the arches of the same name to the dorsal aspect of the posterior part of the tongue.
- 8. TRANSPORT PHASE / ORAL PHASE PROPER • The tongue is moved by the action of the intrinsic muscles together with the genioglossus which elevates tongue tip and blade of the tongue towards the hard palate. • A pre-requisite for this is mandibular elevation . • The elevation of the mandible assists the suprahyoid muscles in raising the hyoid bone. • The elevation of the floor of the mouth is accompanied by lifting the tongue under the action of the stylohyoid.
- 9. • Simultaneously, the tongue is flattened and the bolus is moved back by these muscles together with the superior longitudinal and transversus muscles as the tongue fills the oral cavity • As the bolus reaches the back of the tongue, now deeply grooved, the soft palate is elevated by the levator and tensor veli palatini to protect the nasopharynx from the entry of food and closes the airways.
- 10. The anterior and lateral views of tongue position in holding bolus immediately before initiating oral stage of swallow.
- 11. PHARYNGEAL STAGE • Reflex activity which is initiated as the bolus reaches the back of the tongue.
- 12. • The initiation of swallowing involves contact of the food with the faucial arches or with the mucosa overlying the posterior pharynx in the region that is innervated by the glossopharyngeal nerve. • ‘Trigger point' - summation of afferent signals for the entire oropharyngeal sensory field.
- 13. (a) Closure of nasopharynx - Soft palate contracts against the Passavant’s ridge on the posterior pharyngeal wall and completely cuts off the nasopharynx from the oropharynx. (b) Closure of oropharyngeal isthmus - The entry of food back into oral cavity is prevented by contraction of tongue against the palate and sphincteric action of palatoglossal muscles. (c) Closure of larynx - Aspiration into the larynx is prevented 3-Tier system – 1) Closure of laryngeal vestibule by contraction of aryepiglottic & interarytenoid muscles. 2) Ventricular bands approximation . 3) Adduction of vocal cords by adductors.
- 14. • During this phase, the glottis is closed by adduction of the arytenoids and contraction of the lateral cricoarytenoid muscles, false vocal folds and true vocal folds. • Epiglottis covers the laryngeal entrance and directs the bolus in two parts into the valleculae and the pyriform sinuses. • The two columns of the divided bolus meet at the upper border of the cricopharyngeus muscle which relaxes to allow the bolus to enter the oesophagus.
- 15. • Rapid laryngeal elevation occurs during the pharyngeal phase of the swallow and appears to be essential for normal swallowing. • This manoeuvre produces a drop in pressure and transient negative pressure in the cricopharyngeal sphincter as the bolus passes from the pharynx into the oesophagus.
- 16. Neuromuscular Activities Characteristic of the Pharyngeal Swallow (brainstem) velopharyngeal closure to prevent backflow of material up the nose. tongue base retraction to propel the bolus through the pharynx. pharyngeal contraction to clear residue through the pharynx. airway protection, which involves both elevation and closure of the larynx. cricopharyngeal or upper esophageal sphincter (UES) opening to allow the bolus to pass into the esophagus.
- 18. OESOPHAGEAL PHASE • After food enters the oesophagus, the cricopharyngeal sphincter closes and the peristaltic movements of oesophagus take the bolus down the stomach. • Gastro-oesophageal sphincter at the lower end of oesophagus relaxes well before peristaltic wave reaches and permits fluids to pass. • Bolus of food is passed by contraction of peristaltic waves and then the sphincter closes.
- 19. • The anterior superior movement of the laryngohyoid complex acts to open the upper oesophageal sphincter. • The bolus passes through the sphincter and moves along the oesophagus by peristalsis. • The levator and tensor veli palatini relax lowering the soft palate. • The laryngeal vestibule opens, the hyoid drops and the vocal cords open. • This opening of the glottis at the very end of the oropharyngeal swallow sequence is part of the airway protection mechanism.
- 20. Esophageal Phase (8-20 sec) • Primary peristalsis: Sequential contraction of the circular muscle of the esophageal body, which results in a contractile wave that migrates toward the stomach • Relaxation and opening of the LES • Involuntary control: Vagus • Secondary peristalsis: A peristaltic sequence that occurs in response to distention of the esophagus (not associated with UES relaxation or deglutition)
- 21. • Regurgitation of food back from stomach into oesophagus is prevented by : tone of gastro-oesophageal sphincter. negative intrathoracic pressure. pinch-cock effect of diaphragm. mucosal folds. oesophagogastric angle. slightly positive intra-abdominal pressure
- 22. MOUTH OROPHARYNX CRICOPHARYNGEAL SPHINCTER STOMACH (THROUGH OESOPHAGUS) 1-2 Sec 1 Sec 10-15 Secs TRANSIT TIME
- 23. Oral and pharyngeal stages of a normal swallow: (a) oral phase, food is reduced and the bolus prepared (b) bolus is moved to the posterior part of the tongue (c) bolus contacts the trigger points in the oropharynx and the pharyngeal phase is initiated (d) bolus is moved past the closed larynx (e) Bolus enters the oesophagus.
- 24. RESPIRATION & SWALLOWING (SWALLOW APNOEA) Ventilation has to be suspended during pharyngeal transit of the bolus. Typically less than one second in length, corresponding to the duration of the reflex part of the swallow in its pharyngeal phase. The duration of swallow apnoea is dependent upon bolus volume and possibly bolus consistency.
- 25. • Swallowing tends to occur during the expiration phase of respiration. • Expiration occurs after 80-100 percent of healthy swallows.This is likely to be a protective mechanism: material left in the laryngeal vestibule post swallow will be moved to the pharynx rather than sucked into the lungs. • There does not seem to be an effect of bolus volume or gender on the exhale-swallow-exhale pattern. • The respiratory rhythm is reset after swallowing and there is a shift in the timing of all subsequent breaths post-swallow: type I phase resetting.
- 26. SWALLOW APNOEA
- 27. NEURAL CONTROL • Neural control is divided between the cortex and the brainstem. • Cortical control of swallowing is bilateral, though one hemisphere is usually dominant. • The voluntary initiation of swallowing involves bilateral areas of the prefrontal, frontal and parietal cortices.
- 28. • Positron emission tomography (PET) of the cortex following passive initiation of swallowing reveals activity in several regions like the face areas of both the primary sensory and motor cortex, as well as the prefrontal swallowing areas which are located just anterior to the face region of the precentral gyrus in the primary motor cortex, corresponding to Brodman's area 6. • Stimulation here produces swallowing activity in the appropriate muscles of the oral cavity, pharynx, palate and larynx
- 29. • Afferent input from the jaw, muscles of mastication, lips and tongue, pharynx, larynx , oesophagus. To brainstem, cortex • The efferent pathways (medulla and pons) cranial motor nuclei muscles of swallowing nucleus ambiguus for the muscles of the palate, pharynx and larynx . hypoglossal nucleus for the muscles of the tongue . motor nuclei of the trigeminal and facial nerves for the muscles of the jaws and lips. • In addition, motor neurones within the cervical spinal cord control the muscles of the neck including the infrahyoid.
- 31. Neural Regulation of Swallowing • Pharyngeal: – Stimulation of receptors (7th, 9th, and 10 cranial nerves) – Efferent (motor) function (9th, 10th cranial nerves). Cricopharyngeal sphincter opening is reflexive • Esophageal: – Primary peristalsis • Proximal- striated- contracts first • Distal- smooth- contracts later – Secondary peristalsis • Intrinsic plexus: Auerback’s myentric plexus
- 32. Cranial Nerves • CN V and XII: Chewing & tongue movements. • CN VII: Sensation of oropharynx & taste to anterior 2/3 of tongue . • CN IX: Taste to posterior tongue, sensory and motor functions of the pharynx. • CN X: – Taste to oropharynx, and sensation and motor function to larynx and laryngopharynx. – Airway protection
- 33. • Two main groups of neurones for the coordination and regulation of swallowing by the medulla. The first lies in the dorsal region of the medulla above the nucleus of the solitary tract(lateral medullary swallowing centre). Site of convergence of sensory input from the various nuclei and is probably important in the sequencing of swallowing. A second group lies more ventrally around the nucleus ambiguus (medial medullary swallowing centre). Distributes outputs to the various cranial nerve motor nuclei. (excitatory to agonist muscles and their synergists , inhibitory to the corresponding antagonist muscles).
- 35. • The pharyngeal swallow is mediated in the lower brainstem (the medulla) in the reticular formation immediately adjacent to the respiratory center. • Coordination exists between these two centers because respiration ceases for a fraction of a second when the airway closes during the pharyngeal swallow.
- 37. Pressure changes during deglutition • In oesophagus
- 38. APPLIED PHYSIOLOGY & DISORDERS • PRESBYPHAGIA • ASPIRATION • DYSPHAGIA • ODYNOPHAGIA • MOTILITY DISORDERS
- 39. SPECIAL INVESTIGATIONS • BARIUM SWALLOW • UGI SCOPY • VIDEOFLUOROSCOPY • MANOMETRY • NARROW BAND IMAGING
- 40. REFERENCES • Scott brown’s otorhinolaryngology, head & neck surgery(7TH edition). • Cummings otolaryngology & head & neck surgery (6th edition). • Hazarika textbook of ear,nose ,throat & head & neck surgery (3rd edition). • Dhingra – disaeases of ear , nose, throat & head & neck surgery (6th edition). • Gray’s anatomy (40th edition).