20 Feb 2024
Bifurcation lesions
The PCR-EAPCI Textbook
This updated chapter by T. Lefèvre provides a practical guide on strategies currently implemented in the treatment of coronary bifurcations, and highlights the main challenges and most debated issues to propose recommendations for an optimal approach.
Summary
Coronary bifurcations are by nature prone to the development of atherosclerosis. They pose technical difficulties for percutaneous interventional treatment and they are associated with higher stent thrombosis and restenosis rates. The optimal approach for true coronary bifurcations is still a subject of debate, especially when the side branch (SB) is large, not easily accessible and narrowed by a long lesion. The overall philosophy is to keep it simple and safe, to understand and respect the original anatomy of the bifurcation, to optimize the flow and function of a bifurcation following percutaneous coronary angioplasty and to limit the number of stents which should be well apposed and expanded with limited overlap. The role of dedicated devices in this setting remains unclear. Complex techniques (using two or three stents) should only be used, when necessary, as they are associated with a worse outcome. FKB is strongly recommended when using a complex bifurcation technique.
The consensus of the European Bifurcation Club (EBC) in 2022 is that main branch (MB) stenting with provisional SB stenting should be the default approach in the majority of cases. This approach is associated with a low risk of failure and complications provided that the following guidelines are implemented: wiring of both branches at the beginning of the procedure, stenting of the MB with a stent diameter adapted to the distal MB, immediate optimization of the proximal stent segment according to Finet’s law using the proximal optimization technique (POT). The procedure can be stopped at this point, however, if the SB requires special attention, the POT/side/POT technique or FKB can be used. If SB stenting is necessary, the T, TAP or Culotte technique can be performed. In case of difficult access to the SB, it may be preferable to stent into the SB first using the inverted provisional approach or the Double Kissing Crush (DK Crush) technique following all recommended steps.
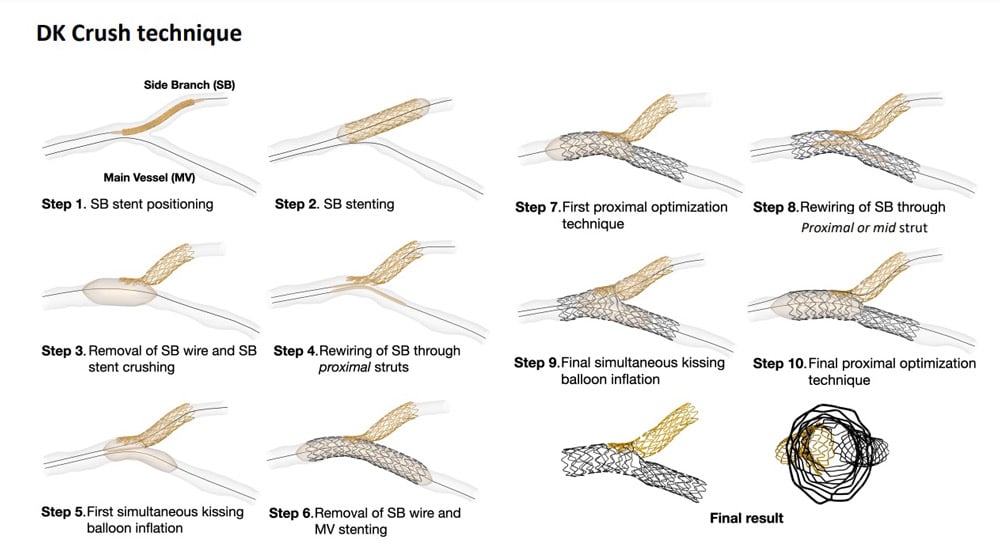
Virtual simulation of the DK CRUSH technique
Authors
Lefèvre T., Hovasse T.
