
Abstract
Dimensionality reduction approaches are commonly used for the deconvolution of high-dimensional metabolomics datasets into underlying core metabolic processes. However, current state-of-the-art methods are widely incapable of detecting nonlinearities in metabolomics data. Variational Autoencoders (VAEs) are a deep learning method designed to learn nonlinear latent representations which generalize to unseen data. Here, we trained a VAE on a large-scale metabolomics population cohort of human blood samples consisting of over 4500 individuals. We analyzed the pathway composition of the latent space using a global feature importance score, which demonstrated that latent dimensions represent distinct cellular processes. To demonstrate model generalizability, we generated latent representations of unseen metabolomics datasets on type 2 diabetes, acute myeloid leukemia, and schizophrenia and found significant correlations with clinical patient groups. Notably, the VAE representations showed stronger effects than latent dimensions derived by linear and non-linear principal component analysis. Taken together, we demonstrate that the VAE is a powerful method that learns biologically meaningful, nonlinear, and transferrable latent representations of metabolomics data.
Similar content being viewed by others


Introduction
Modern metabolomics experiments yield high-dimensional datasets with hundreds to thousands of measured metabolites in large human studies with thousands of participants1. Such datasets are routinely generated to profile the molecular phenotype of disease and identify the underlying pathological mechanisms of action2,3,4,5. Extracting systemic effects from high-dimensional datasets requires dimensionality reduction approaches to untangle the high number of metabolites into the processes in which they participate. To this end, linear dimensionality reduction methods, such as principal component analysis (PCA) and independent component analysis (ICA), have been extensively applied to high-dimensional biological data6,7,8,9,10. However, metabolic systems, like most complex biological processes, contain non-linear effects which arise due to high-order enzyme kinetics and upstream gene regulatory processes11,12. For example, metabolite ratios are an intuitive and widely used approach to detect non-linear effects in metabolomics data, approximating the steady state between reactants and products of metabolic reactions13,14. Extending this concept, systematic methods that take nonlinearities into account are required to correctly recover the functional interplay between metabolites in an unbiased fashion.
Autoencoders (AEs) are a type of neural network architecture developed as an unsupervised dimensionality reduction method that can capture non-linear effects15. AEs reduce high-dimensional data into latent variables through an encoding/decoding process which recreates the input data after passing through a lower dimensional space. Once the model is fitted, the latent variables represent a compact, often easier-to-interpret version of the original data. While AEs have been successfully used for prediction tasks on biological datasets16, they tend to learn latent spaces specifically fitted to the input dataset and are therefore not generalizable to biological phenomena absent from the training data17. To address this, Variational Autoencoders (VAEs) were introduced as a probabilistic extension of the AE architecture that constrains the latent variables to follow a predefined distribution18. With this extension, the VAE not only reconstructs the input data, but infers the generative process behind the data, leading to high generalizability across datasets. The VAE architecture has, for example, proven effective for predicting cell-level response to infection from transcriptomic data in cell types not used during training, and predicting drug response from gene expression data where drug response information was sparse17,19,20. In addition, latent dimensions of VAE models trained on gene expression data have been shown to strongly associate with clinical parameters21 and have outperformed other common low-dimensional representation methods (PCA and k-means clustering) in capturing biologically meaningful pathways22.
The application of deep learning architectures to metabolomics datasets has considerably lagged behind most other omics23 due to the unavailability of large metabolomics cohorts. One previous study used (non-variational) AEs on a small set of metabolomics samples (n = 271), demonstrating superior predictability of ER status in breast cancer patients using the latent representations of the model over common machine learning methods24. By applying VAE architectures to large-scale metabolomics data, we have the potential to learn more accurate latent dimension representations that systematically account for non-linear effects. In addition, the probabilistic structure of VAEs will learn latent dimensions that are generalizable across multiple datasets.
In this paper, we trained a VAE model on 217 metabolite measurements in 4644 blood samples from the TwinsUK study25 and evaluated our model performance in comparison to linear and non-linear PCA models (Fig. 1a). To investigate the biological relevance of the learned VAE and PCA latent dimensions, we employed the Shapley Additive Global Importance (SAGE) method26, which determines the contribution of each input to each latent dimension. We calculated SAGE values at different granularities, i.e., metabolites, sub-pathways, and super-pathways (Fig. 1b). We then applied the models on three additional blood metabolomics datasets to test their ability to recover disease phenotypes in unseen datasets: Type 2 Diabetes diagnosis in The Qatar Metabolomics Study on Diabetes (QMDiab, n = 358), therapy response in an acute myeloid leukemia dataset (AML, n = 85), and schizophrenia diagnosis in a third validation dataset (n = 201) (Fig. 1c).

a VAE, linear PCA, and non-linear kernel (K)PCA models were trained using training and test sets in the TwinsUK dataset (n = 4644 samples, p = 217 metabolites). Model performance was then evaluated using Mean Squared Error (MSE) of metabolite correlation matrix reconstruction. b The SAGE method was applied to calculate the contribution of individual metabolites, sub-pathways and super-pathways to each latent dimension. c QMDiab (n = 358), AML (n = 85), and Schizophrenia (n = 201) datasets were encoded using VAE and PCA models trained on the TwinsUK data. Latent dimensions of each model were then associated with disease phenotypes.
Results
VAE model construction and fitting
Our VAE architecture consisted of an input/output layer, an intermediate layer and a latent layer. We split the TwinsUK cohort into an 85% training and a 15% test set, and the training set was used to optimize the hyperparameters in the VAE model. Keras Tuner27 identified the following optimal hyperparameters: Intermediate layer dimensionality = 200, learning rate = 0.001, and Kullback-Leibler (KL) divergence weight = 0.01 (see Methods). With these parameters fixed, we optimized the dimensionality d of the latent layer z by calculating the reconstruction MSE of the correlation matrix (CM-MSE) of metabolites (Fig. 2a, b). We observed that the CM-MSE curve plateaus after d = 18, indicating that increasing the latent dimensionality beyond this value only marginally improved the models. The final architecture of the model consisted of a 217-dimensional input/output layer (the number of metabolites in our datasets), a 200-dimensional intermediate layer, and an 18-dimensional latent layer (Fig. 2c).

a Training and b test set metabolite correlation matrix reconstruction for a range of latent dimensionality values d. The slope of the VAE curve plateaued after d = 18. Error bars correspond to one standard deviation from bootstrapping (n = 1000 iterations). c Final VAE architecture, where μ is the mean vector and σ is the standard deviation vector that generates the latent space z. d Reconstruction MSE for latent dimensionality d = 18 on training and test sets. The box represents the interquartile range (IQR), whiskers are up to 1.5x IQR, and plotted points are outliers. The VAE preserved feature correlations substantially better than PCA. Kernel PCA-based results can be found in Supplementary Figs 3 and 4.
We used principal component analysis (PCA) as a baseline model to compare the VAE to a linear latent variable embedding method. To this end, we fitted a PCA on the TwinsUK train data and extracted the first d = 18 dimensions, i.e., principal components. To further compare our VAE results to a non-linear latent variable method, we used the same fit and extraction procedures using kernel (K)PCA models with cosine similarity, sigmoid, RBF, and polynomial kernel transformations. On training data, neither PCA nor VAE outperformed KPCA data matrix reconstruction. On testing data, however, both PCA and VAE outperformed the KPCA models, with PCA showing better reconstruction accuracy of the data matrix than the VAE (Supplementary Figs 1 and 2). All non-linear models, KPCA and VAE, outperformed PCA in correlation matrix reconstruction via CM-MSE in both the TwinsUK train and test set (Fig. 2d, Supplementary Fig. 3).
This difference between the MSE on the correlation matrix and the more commonly used sample-wise MSE18 outlines ambiguities in the methods to assess reconstruction performances. Notably, other authors have shown previously that sample reconstruction performance does not necessarily imply better model performance19,20, as evidenced by the large discrepancy of KPCA sample reconstruction between training and test sets. However, our results suggest that while the non-linear methods do not reconstruct the original data matrix precisely, they are superior to PCA at preserving metabolite correlations.
Interpretation of VAE latent space dimensions in the context of metabolites and pathways
We evaluated the composition of all latent dimensions in the context of metabolic pathways. For each metabolite in our dataset, a “sub-pathway” and “super-pathway” annotation was available (see Methods). Sub-pathways refer to biochemical processes such as “TCA Cycle” and “Sphingolipid Metabolism”, while super-pathways are broad groups such as “Lipid” and “Amino acid”. To provide insights into the processes represented by different VAE dimensions, we computed SAGE scores26, a measure of model feature relevance, at the level of metabolites, sub-pathways and super-pathways (Fig. 3 and Supplementary Fig. 4). PCA and KPCA results can be found in Supplementary Figs 5–9.

a SAGE values were scaled by dimension, i.e., set to standard deviation 1 for each column in the matrix. This highlights pathways that contributed the most to each dimension. Lipid and amino acid super-pathways showed the highest values for most dimensions, which can be attributed to the high number of metabolites in those pathways. b SAGE values were scaled by pathway, i.e., set to standard deviation 1 for each row in the matrix. This highlights dimensions that contributed to a pathway the most. Taking into consideration the largest scaled SAGE values per pathway (red square marks), almost all sub-pathways were represented by unique dimensions. The combination of these key sub-pathways of a dimension outlined the distinct cellular mechanisms a dimension encodes.
The VAE sub-pathway heatmap (Fig. 3a) shows that nearly all dimensions have major contributions by lipid and amino acid super-pathways. The prevalence of the two super-pathways can be attributed to the fact that those groups contain the largest number of metabolites in the dataset. Note that we deliberately omitted the “Unknown” molecule group, which refers to unidentified metabolites that could originate from any pathway.
Inspecting the SAGE values in the other direction, almost all sub-pathways are predominantly represented by a single VAE dimension that captures the respective pathway the most (Fig. 3b, red square marks). For instance, “glycolysis, gluconeogenesis and pyruvate metabolism” is functionally related to the sub-pathway pathway “Alanine and Aspartate Metabolism” through the glucose-alanine cycle28, and both were represented by VAE dimension 12. Another interesting example is VAE dimension 14, which captured essential catabolic processes, such as ketone bodies, fatty acid metabolism, and the TCA cycle. Taken together, these results show that VAE latent dimensions capture a complex mix of functionally related sub-pathways, thus capturing major metabolic processes in the dataset.
In contrast, PCA and KPCA dimensions 1 to 5, which by construction represent the highest variations in the data, nonspecifically captured various sub-pathways. Most other PCA and KPCA dimensions also primarily contained unrelated sub-pathways (Supplementary Figs 5–9).
VAE latent space captures signals in unseen diabetes, schizophrenia, and cancer metabolomics datasets
We investigated whether VAE latent dimensions learned on the TwinsUK data contained information that is generalizable to other datasets. To this end, we encoded metabolomics data from three clinical datasets, type 2 diabetes, acute myeloid leukemia (AML), and schizophrenia using the VAE, PCA, and KPCA encoders trained on the TwinsUK dataset. For each VAE, PCA, and KPCA latent dimension, we performed a two-sided t-test between diabetic vs. non-diabetic individuals, full vs. no response in an AML clinical trial, and schizophrenic vs. non-schizophrenic individuals, respectively. Across all datasets, the best performing VAE dimensions associated substantially stronger with the patient groups than any of the PCA or KPCA dimensions (Fig. 4a–f). The strength of associations between VAE dimensions and disease parameters were comparable to single metabolite associations (Supplementary Data 1 and 2). However, unlike the VAE dimensions, these univariate associations do not represent system-level mechanisms related to the diseases. Notably, results did not differ substantially for different dimensionalities than d = 18 (Supplementary Fig. 15).

a–c Sorted −log10(p-value) for all VAE, PCA and KPCA dimensions for the type 2 diabetes (n = 358), AML (n = 85), and schizophrenia (n = 201) datasets, respectively. The highest scoring VAE dimensions showed lower p-values than the highest scoring KPCA dimensions, and considerably lower p-values than the highest scoring PCA dimensions for all datasets. d–f Boxplots of latent dimension values for latent space dimensions with the lowest p-values for the three datasets. The box represents the interquartile range (IQR), whiskers are up to 1.5x IQR, and plotted points are outliers. g Contributions of super-pathways, sub-pathways and metabolites determined by SAGE values to dimension 12, the highest scoring VAE latent dimension for QMDiab and AML. This dimension was driven by lipids, amino acids, and carbohydrates. h Contributions of super-pathways, sub-pathways and metabolites determined by SAGE values to dimension 11, the highest scoring VAE latent dimension for Schizophrenia. This dimension was largely driven by amino acid metabolism. p = p-value. Schizo. = schizophrenic.
To obtain a better understanding of the driving factors of the VAE associations, we ranked pathways and metabolites by their calculated SAGE values (Fig. 4g–i):
Type 2 diabetes
VAE latent dimension 12 showed the highest association with type 2 diabetes, with a considerably stronger signal than the second highest association by PCA dimension 16 (p = 1.6 × 10−22 vs. p = 2.1 × 10−20, respectively; Fig. 4d). The top sub-pathways were “glycolysis, gluconeogenesis, and pyruvate metabolism”, “Lysolipid”, and “Glycine, Serine, and Threonine metabolism”. The top-ranking metabolite in dimension 12 was glucose, which is a main factor directly affected by the disease, and thus served as a positive control. Other high-ranking metabolites included serine, mannose, and glycine (Fig. 4g). Reduced levels of the glucogenic amino acids serine and glycine have repeatedly been reported in Type 2 Diabetes cases as impaired glucose uptake in insulin-resistant cells triggers hepatic gluconeogenesis, consuming these amino acids29,30,31. Furthermore, plasma levels of mannose have also been found to associate with type 2 diabetes diagnosis32. We then correlated dimension 12 with clinical lab measurements from the QMDiab study and found a strong association between this dimension and HbA1c, a widely used diabetes biomarker33,34 (p = 6.2 × 10−45 compared to PCA p = 1.1 × 10−30, and the strongest associated KPCA dimension p = 6.0 × 10−38, Supplementary Figs 10–12). This finding demonstrates how a quantitative disease biomarker can carry more information than a crude disease yes/no classification, and further highlights the higher information content in the VAE latent dimensions compared to PCA.
Acute myeloid leukemia (AML)
AML response groups associated an order of magnitude stronger with VAE dimension 12 than with RBF KPCA dimension 10 (p = 0.027 vs. p = 0.12, respectively; Fig. 4f). Note that the p-value would not withstand multiple testing correction (Supplementary Data 1); the detected signal is thus merely suggestive and requires replication in future studies. In addition to the glycolytic signals described above, dimension 12 was also driven largely by the “Lipid” super-pathway, with the “Lysolipid” sub-pathway ranking highly for this dimension. The lysolipid sub-pathway has prominent contributions from the metabolite 1-palmitoleyolglycerophosphocholine, belonging to the glycerophosphocholine (GPC) family, which are products of cellular membrane breakdown35. In the clinical trial from which the AML data was taken, the clinical arms were given varying doses of the drug daunorubicin, an anthracycline antibiotic whose mechanism of action includes targeting the cell membrane36,37,38,39. In fact, the localization of daunorubicin in cellular membranes depends on the daunorubicin/lipid ratio, and therefore differential lipid concentrations between patients could affect drug response40,41. In addition, the sub-pathway “Polyunsaturated Fatty Acid (n3 and n6)” was another lipid-related driver of dimension 12. The upregulation of polyunsaturated fatty acids (PUFA) is a trait of anthracyclin treatment42, indicating that differential abundance of PUFA may reflect treatment efficacy and thus response in the clinical trial arms. We furthermore investigated correlations of the latent dimensions with 21 major AML-related mutations; the analysis revealed only one significant result, with the NPM1 mutation associating significantly with polynomial KPCA model dimension 11 (t-test, p < 0.05, Supplementary Figs 13 and 14). However, this genetic association did not translate to the clinical association with drug response.
Schizophrenia
VAE dimension 11 had a stronger association with schizophrenia than the second-ranked RBF KPCA dimension 2 (p = 3.0 × 10−6 vs. p = 3.6 × 10−6, respectively; Fig. 4e). The top scoring super-pathway for this dimension (Fig. 4h) was amino acids, with the Phenylalanine and Tyrosine metabolism sub-pathway and its associated metabolites 3-(4-hydroxyphenyl)lactate, phenyllactate (PLA), and tyrosine being highly ranked in this dimension. Phenylalanine and tyrosine are the amino acid precursors for the synthesis of the main neurotransmitter implicated in the neurobiology of schizophrenia, dopamine43. Many studies have shown altered transport of tyrosine across the blood-brain barrier as a prominent mechanism in schizophrenic patients44,45,46. In addition, inflammation, increasingly implicated in schizophrenic patients, reduces the activity of the enzyme responsible for converting phenylalanine to tyrosine, such that phenylalanine is instead converted to phenylpyruvic acid, a precursor metabolite to PLA43,47. Finally, dimension 11 was strongly driven by the amino acid creatine. Studies have shown that schizophrenia patients have significantly reduced brain levels of creatine compared with healthy controls48, and creatine-producing enzymes in serum have long been implicated in schizophrenic psychosis49,50.
Taken together, these results suggest that our VAE has learned representations of metabolic processes that are essential in unseen clinical outcomes.
Discussion
In this study, we trained a VAE on metabolomics data from the TwinsUK population cohort and applied the learned latent representations on unseen data. Notably, non-linear dimensionality reduction methods, including kernel PCA and our VAE model, outperformed the linear PCA model in metabolite correlation matrix reconstruction, underlining the importance of non-linear relationships in metabolomics data. Interpretation of VAE latent dimensions at the metabolite, sub-pathway, and super-pathway level revealed that these dimensions represent functionally related and distinct cellular processes. Moreover, VAE latent dimensions showed substantially stronger disease associations than PCA and even the non-linear KPCA models in unseen Type 2 Diabetes, AML, and schizophrenia datasets. This demonstrates that the VAE learned a latent representation of metabolomics data that is biologically informative and transferable across different cohorts.
The generalizability of the VAE across different datasets is especially remarkable given the vastly different underlying populations of the datasets analyzed here. The VAE was trained on the TwinsUK population cohort, a European-ancestry population cohort consisting predominantly of British women (~92%), while the validation datasets are mixed-gender and multi-ethnic cohorts from the US and Qatar. Despite the existence of these variations in our datasets, our VAE learned a generalized representation of metabolomics data which was able to identify disease-related differences.
The main limitation of our study is the size of the TwinsUK training dataset with n = 4644. This is a general issue with human subject metabolomics studies, where even the largest cohorts reach only about n = 15,00051. Deep learning models are currently more popular in larger datasets of n = 60,000 samples or more, such as single cell transcriptomic52,53,54,55, image56,57,58, and text sources59. Learning the variation in such large datasets allows these models to significantly outperform their linear counterparts. Large metabolomics datasets, such as that of the UK BioBank with a sample size of up to n = 500,00060, will be available in the near future, and will enable the creation of more expressive and deeper VAE models.
To the best of our knowledge, this is the first study to construct a universal latent representation of large-scale metabolomics data using VAEs. Our results show that VAEs are well-suited for metabolomics data analysis and can potentially replace dimensionality reduction approaches, such as PCA, in creating a universal, systems-level understanding of metabolism.
Methods
Datasets
The TwinsUK registry is a population-based study of around 12,000 volunteer twins from all over the United Kingdom. The participants have been recruited since 1992 and are predominantly female, ranging in age from 18 to 103 years old25. For our study, we included data from 4644 twins (4256 females, 388 males), the subset of TwinsUK for which plasma metabolomics measurements were available. Ethical approval was granted by the St Thomas’ Hospital ethics committee and all participants provided informed written consent.
The QMDiab study was conducted between February and June of 2012 at the Dermatology Department of Hamad Medical Corporation (HMC) in Doha, Qatar. The study population was between the ages of 23 and 71, predominantly of Arab, South Asian, and Filipino descent61. For this study, we included plasma data of 358 subjects (176 females, 182 males; 188 diabetic, 177 non-diabetic). The study was approved by the Institutional Review Boards of HMC and Weill Cornell Medicine-Qatar (WCM-Q). Written informed consent was obtained from all participants.
The cohort of patients with acute myeloid leukemia (AML) comes from the ECOG-ACRIN Cancer Research Group phase 3 trial NCT00049517. This study was conducted between December 2002 and November 2008, recruiting 657 patients with AML between the ages of 17 and 60. A subset of these patients had follow-up profiling to determine their response to therapy. For this study, we included the serum metabolomics measurements of 85 subjects of which 43 responded to therapy and 42 did not (34 females, 51 males). The study was approved by the institutional review board at the National Cancer Institute and each of the study centers, and written informed consent was provided by all patients.
For the schizophrenia analysis, metabolomics samples were taken from an antipsychotics study conducted in Qatar between December 2012 and June 201462. A total of 226 participants between the ages of 18 and 65 years of age were recruited, predominantly of Arab descent. For our study, we included plasma metabolomics measurements from 201 subjects (76 females, 125 males; 97 schizophrenic, 104 non-schizophrenic). Approval for the study was obtained from the HMC and WCM-Q Institutional Review Boards, and all participants provided written informed consent.
Metabolomics measurements and metabolite annotations
Metabolic profiling for all four cohorts was performed using non-targeted ultrahigh-performance liquid chromatography and gas chromatography separation, coupled with mass spectrometry on the Metabolon Inc. platform as previously described63. Notably, the AML dataset was based on serum samples, while TwinsUK, QMDiab, and schizophrenia metabolomics were run on plasma samples. However, previous studies have shown that these two sample types are comparable, as shown by high correlations and good reproducibility between plasma and serum measurements in the same blood sample64.
For each metabolite measured on the Metabolon platform, a super-pathway and sub-pathway annotation was provided. For super-pathways, we have nine annotations referring to broad biochemical classes, namely “Amino acid”, “Carbohydrate”, “Cofactors and vitamins”, “Energy”, “Lipid”, “Nucleotide”, “Peptide”, “Xenobiotics”, and “Unknown”. Note that “Unknown” is assigned to unidentified metabolites. Furthermore, we have 54 sub-pathway which represent more functional metabolic processes, such as “Carnitine metabolism”, “TCA Cycle”, and “Phenylalanine and Tyrosine Metabolism”.
Data processing and normalization across datasets
For each dataset, metabolite levels were scaled by their cohort medians, quotient normalized58 and then log-transformed. Samples with more than 30% missing metabolites and metabolites with more than 10% missing samples were removed. Missing values were imputed using a k-nearest neighbors imputation method65. Datasets with BMI measurements (Schizophrenia, QMDiab, and Twins) were corrected for that confounder and then mean-scaled. 217 metabolites were overlapping between the 4 datasets and were kept for further analysis.
Semi-quantitative, non-targeted metabolomics measurements are inherently challenging to compare across datasets due to heterogeneity between studies. This prevents any machine learning model from being directly transferable from one study to the other. Thus, to ensure comparability, datasets were normalized using a uniform group of participants as a reference set. This group was selected as follows: Male, within a 20-year age range (30–50 for TwinsUK, QMDiab, and schizophrenia, 40–60 for AML due to low sample size of younger participants), BMI between 25 and 30 (not available for AML data, thus not filtered for that dataset), and in the respective control group. Each metabolite in each dataset was then scaled by the mean and standard deviation of their respective uniform sample groups. The assumption of this approach is that the uniform group of reference participants has the same distributions of metabolite concentrations.
Variational autoencoder fitting
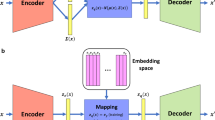
To train our VAE model, we first split the TwinsUK data into 85% training and 15% test sets. We then fixed our VAE architecture to be composed of an input/output layer, an intermediate layer which contains non-linear activation functions, and a d-dimensional latent layer. The latent layer consists of a mean vector μ and a standard deviation vector σ, both of length d, which parametrize each latent dimension as a Gaussian probability distribution. This latent space, denoted by z, is constructed by the simultaneous learning of the μ and σ encoder through the use of a reparameterization trick that enables back propagation during training18. The d x d covariance matrix ∑ of the underlying multivariate Gaussian is assumed to be diagonal (i.e., no correlation across latent dimensions), allowing the covariance matrix to be represented by a single vector σ of length d.
For the parameter fitting procedures, all weights were initialized using Keras’ default model weight initialization, i.e., Glorot uniform66. Leaky rectified linear units (ReLUs)67 were used for non-linear activation functions. The VAE models were trained for 1000 epochs using MSE loss for sample reconstruction and a batch size of 32.
To select the latent dimensionality d of our VAE model, we initially fixed this value to d = 50. We then optimized the model hyperparameters using Keras Tuner27 and the TwinsUK training set with MSE as the objective metric to minimize. We identified the following optimized values: Intermediate layer dimensionality = 200, learning rate = 0.001, and Kullback-Leibler (KL) divergence weight = 0.01. Note that despite our hyperparameter choices, other optimal hyperparameters exist and could be chosen through Keras Tuner. Using these hyperparameters, we then optimized d by calculating the reconstruction MSE of the correlation matrix (CM-MSE) of metabolites for d = 5, 10, 15, 18, 20, 30, 40, 60, 80, 100, 120, 160, and 200 on the TwinsUK test set. Our final model consisted of a 217-dimensional input/output layer (the number of metabolites in our datasets), a 200-dimensional intermediate layer, and an 18-dimensional latent layer. For all sample encodings in the study, we used their respective μ values.
We further performed sensitivity analysis to determine the effect of the choice of d on clinical parameter association. We trained 100 models using the architecture above, varying the latent layer dimensionality for d = 10, 13, 15, 16, 17, 18, and 20. For each model, we extracted the p-value of the highest associated latent dimension, creating a p-value distribution for each d, which was then compared to the PCA and KPCA associations (Supplementary Fig. 15).
All models were computed on a deep learning-specific virtual machine running on Google Compute Engine with two NVIDIA Tesla K80 GPU dies and 10 virtual CPUs.
PCA and kernel PCA embedding and reconstructions
We used PCA with d = 18 latent dimensions as a baseline model. On the mean-centered TwinsUK training set data matrix with n = 3947 samples (rows) and k = 217 metabolites (columns), we calculated the rotation matrix Q, a k x k matrix of eigenvectors ordered by decreasing magnitudes of eigenvalues. To embed a new m x k dataset X with m samples into the m x d PCA latent space A, we first calculated XQ = A and subsetted to the first d columns, denoted by A∗, d. To simulate the process of encoding and decoding in PCA for dataset X, we calculated the reconstructed dataset as
We used kernel PCA with d = 18 latent dimensions as comparative non-linear models. Using the Scikit-learn python package68, we applied the four available non-linear kernels to the mean-centered TwinsUK training set data matrix: cosine similarity, sigmoid, radial basis function (RBF), an d polynomial transformations. KPCA hyperparameters were chosen for each individual kernel using the grid search method based on their ability to minimize model MSE. Once transformed, the decomposition, embedding, and encoding/decoding processes were performed identically to those of linear PCA.
Model assessments
We assessed our KPCA, PCA and VAE models using sample reconstruction mean squared error (MSE) and metabolite-wise correlation matrix MSE (CM-MSE). We calculated CM-MSE by first computing the metabolite-wise correlation matrix of an input dataset and reconstructed input dataset. Afterwards, we calculated the MSE between the upper triangular matrix of the two symmetric correlation matrices.
To calculate a confidence interval for both MSE and CM-MSE between our input and reconstructed data, we randomly sampled the same samples with replacement from the two datasets and then calculated MSE and CM-MSE. We performed this for 1000 iterations.
Model interpretation
In order to interpret each latent dimension for our VAE, PCA, and KPCA models, we calculated Shapley Additive Global Importance (SAGE) values26 for metabolites, sub-pathways, and super-pathways. As contributions of metabolites, sub-pathways, and super-pathways to latent dimensions can vary between multiple trained VAE models, this analysis was performed on a VAE model with average performance from the clinical association analysis. Briefly, SAGE is a model-agnostic method that quantifies the predictive power of each feature in a model while accounting for interactions between features. This is achieved by quantifying the decrease in model performance when combinations of model variables are removed. Since there are exponentially many combinations of variables, a common approach is to sample the feature combination space sufficiently. For each of the tested combinations, a loss function, such as MSE, is used to quantify the decrease in performance compared to the model output (here each VAE, PCA, and KPCA latent dimension) computed using the full model. Then, the mean of all MSEs is calculated, which represents the contribution of the model variables to a latent dimension. To calculate pathway-level SAGE values, metabolites were grouped into pathways and each pathway was treated as a single variable. For each of our VAE, PCA, and KPCA models, we ran SAGE using our TwinsUK test set with default parameters, e.g., marginal sampling size of 512, as suggested by Covert, et al. 26. We used the SAGE code from https://github.com/iancovert/sage.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
Type 2 diabetes (QMDiab), acute myeloid leukemia (AML), and schizophrenia datasets used in this study are deposited at (https://figshare.com/s/6716415ce4b4e8295f5b). The TwinsUK dataset can be accessed via https://twinsuk.ac.uk/resources-for-researchers/access-our-data/ upon request.
Code availability
Codes used in this study are available at the GitHub repository https://github.com/krumsieklab/mtVAE and https://doi.org/10.5281/zenodo.653307869.
References
Zampieri, M., Sekar, K., Zamboni, N. & Sauer, U. Frontiers of high-throughput metabolomics. Curr. Opin. Chem. Biol. 36, 15–23 (2017).
Bobrovnikova-Marjon, E. & Hurov, J. B. Targeting metabolic changes in cancer: Novel therapeutic approaches. Annu. Rev. Med. 65, 157–170 (2014).
Inoue, K. et al. Metabolic profiling of Alzheimer’s disease brains. Sci. Rep. 3, 2364 (2013).
De Preter, V. et al. Metabolic profiling of the impact of oligofructose-enriched inulin in Crohn’s disease patients: A double-blinded randomized controlled trial. Clin. Transl. Gastroenterol. 4, e30 (2013).
Hartiala, J. A. et al. Genome-wide association study and targeted metabolomics identifies sex-specific association of CPS1 with coronary artery disease. Nat. Commun. 7, 10558 (2016).
Liu, Y. et al. MetICA: Independent component analysis for high-resolution mass-spectrometry based non-targeted metabolomics. BMC Bioinformatics 17, 114 (2016).
Krumsiek, J., Suhre, K., Illig, T., Adamski, J. & Theis, F. J. Bayesian Independent Component Analysis Recovers Pathway Signatures from Blood Metabolomics Data. J. Proteome Res. 11, 4120–4131 (2012).
Nyamundanda, G., Brennan, L. & Gormley, I. C. Probabilistic principal component analysis for metabolomic data. BMC Bioinformatics 11, 571 (2010).
Yamamoto, H. et al. Dimensionality reduction for metabolome data using PCA, PLS, OPLS, and RFDA with differential penalties to latent variables. Chemom. Intell. Lab. Syst. 98, 136–142 (2009).
Teschendorff, A. E., Journée, M., Absil, P. A., Sepulchre, R. & Caldas, C. Elucidating the altered transcriptional programs in breast cancer using independent component analysis. PLoS Comput. Biol. 3, 1539–1554 (2007).
Schwahn, K., Beleggia, R., Omranian, N. & Nikoloski, Z. Stoichiometric correlation analysis: Principles of metabolic functionality from metabolomics data. Front. Plant Sci. 8, 2152 (2017).
Song, H.-S. & Ramkrishna, D. Complex Nonlinear Behavior in Metabolic Processes: Global Bifurcation Analysis of Escherichia coli Growth on Multiple Substrates. Processes 1, 263–278 (2013).
Illig, T. et al. A genome-wide perspective of genetic variation in human metabolism. Nat. Genet. 42, 137–141 (2010).
Petersen, A. K. et al. On the hypothesis-free testing of metabolite ratios in genome-wide and metabolome-wide association studies. BMC Bioinformatics 13, 120 (2012).
Kramer, M. A. Nonlinear principal component analysis using autoassociative neural networks. AIChE J. 37, 233–243 (1991).
Lemsara, A., Ouadfel, S. & Fröhlich, H. PathME: pathway based multi-modal sparse autoencoders for clustering of patient-level multi-omics data. https://doi.org/10.1186/s12859-020-3465-2
Lotfollahi, M., Wolf, F. A. & Theis, F. J. scGen predicts single-cell perturbation responses. Nat. Methods 16, 715–721 (2019).
Kingma, D. P. & Welling, M. Auto-encoding variational bayes. in 2nd International Conference on Learning Representations, ICLR 2014 - Conference Track Proceedings (International Conference on Learning Representations, ICLR, 2014).
Rampášek, L., Hidru, D., Smirnov, P., Haibe-Kains, B. & Goldenberg, A. Dr.VAE: Improving drug response prediction via modeling of drug perturbation effects. Bioinformatics 35, 3743–3751 (2019).
Rampasek, L., Hidru, D., Smirnov, P., Haibe-Kains, B. & Goldenberg, A. Dr. VAE: Drug response variational autoencoder. Bioinformatics. 35, 3743–3751 (2017).
Way, G. P., Zietz, M., Rubinetti, V., Himmelstein, D. S. & Greene, C. S. Compressing gene expression data using multiple latent space dimensionalities learns complementary biological representations. Genome Biol. 21, 109 (2020).
Dincer, A. B., Celik, S., Hiranuma, N. & Lee, S. I. DeepProfile: Deep learning of cancer molecular profiles for precision medicine. Preprint at https://www.biorxiv.org/content/10.110 (2018).
Pomyen, Y. et al. Deep Metabolome: Applications of deep learning in metabolomics. Comput. Struct. Biotechnol. J. 18, 2818–2825 (2020).
Alakwaa, F. M., Chaudhary, K. & Garmire, L. X. Deep Learning Accurately Predicts Estrogen Receptor Status in Breast Cancer Metabolomics Data. J. Proteome Res. 17, 337–347 (2018).
Moayyeri, A., Hammond, C. J., Hart, D. J. & Spector, T. D. The UK adult twin registry (twinsUK resource). Twin Res. Hum. Genet. 16, 144–149 (2013).
Covert, I., Lundberg, S. & Lee, S.-I. Understanding Global Feature Contributions With Additive Importance Measures. NIPS’20: Proceedings of the 34th International Conference on Neural Information Processing Systems. 1444, 17212–17223 (2020).
O’Malley, T. et al. Keras Tuner. (2019). https://github.com/keras-team/keras-tuner
Felig, P. The Glucose-Alanine Cycle. Metabolism 22, 179–207 (1973).
Altmaier, E. et al. Bioinformatics Analysis of Targeted Metabolomics—Uncovering Old and New Tales of Diabetic Mice under Medication. Endocrinology 149, 3478–3489 (2008).
Gall, W. E. et al. α-Hydroxybutyrate Is an Early Biomarker of Insulin Resistance and Glucose Intolerance in a Nondiabetic Population. PLoS One 5, e10883 (2010).
Michaliszyn, S. F. et al. Metabolomic profiling of amino acids and β-cell function relative to insulin sensitivity in youth. J. Clin. Endocrinol. Metab. 97, E2119–24 (2012).
Mardinoglu, A. et al. Plasma Mannose Levels Are Associated with Incident Type 2 Diabetes and Cardiovascular Disease. Cell Metab. 26, 281–283 (2017).
Nathan, D. M. et al. International expert committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 32, 1327–1334 (2009).
Diagnosis and classification of diabetes mellitus. Diabetes Care 33, S62–S69, (2010).
Glunde, K., Ackerstaff, E., Mori, N., Jacobs, M. A. & Bhujwalla, Z. M. Choline Phospholipid Metabolism in Cancer: Consequences for Molecular Pharmaceutical Interventions. https://doi.org/10.1021/mp060067e (2006).
Abdella, B. R. J. & Fisher, J. A chemical perspective on the anthracycline antitumor antibiotics. Environmental Health Perspectives VQl. 64, 4–18 (1985).
Escriba, P. V., Sastre, M. & Garcia-Sevilla, J. A. Disruption of cellular signaling pathways by daunomycin through destabilization of nonlamellar membrane structures. Proc Natl Acad Sci U S A 92, 7595–7599 (1995).
Escribá, P. V. Membrane-lipid therapy: A new approach in molecular medicine. Trends Mol. Med. 12, 34–43 (2006).
Alves, A. C. et al. A biophysical approach to daunorubicin interaction with model membranes: relevance for the drug’s biological activity. https://doi.org/10.1098/rsif.2017.0408
Ferrer-Montiel, A. V., Gonzalez-Ros, J. M. & Ferragut, J. A. Association of daunomycin to membrane domains studied by fluorescence resonance energy transfer. Biochim. et Biophys. Acta. 937, 379–386 (1988).
Heywang, C., Chazalet, M. S. P., Masson, M. & Bolard, J. Orientation of anthracyclines in lipid monolayers and planar asymmetrical bilayers: A surface-enhanced resonance raman scattering study. Biophys. J. 75, 2368–2381 (1998).
Balgoma, D. et al. Anthracyclins Increase PUFAs: Potential Implications in ER Stress and Cell Death. https://doi.org/10.3390/cells10051163 (2021).
Okusaga, O. et al. Elevated Levels of Plasma Phenylalanine in Schizophrenia: A Guanosine Triphosphate Cyclohydrolase-1 Metabolic Pathway Abnormality? PLoS One 9, e85945 (2014).
Wiesel, F. A., Venizelos, N., Bjerkenstedt, L. & Hagenfeldt, L. Tyrosine transport in schizophrenia. Schizophr. Res. 13, 255–258 (1994).
Flyckt, L. et al. Aberrant Tyrosine Transport Across the Cell Membrane in Patients With Schizophrenia. Arch. Gen. Psychiatry 58, 953–958 (2001).
Bjerkenstedt, L. et al. Support for limited brain availability of tyrosine in patients with schizophrenia. Int. J. Neuropsychopharmacol. 9, 247–255 (2006).
Sarkissian, C. N., Scriver, C. R. & Mamer, O. A. Measurement of phenyllactate, phenylacetate, and phenylpyruvate by negative ion chemical ionization-gas chromatography/mass spectrometry in brain of mouse genetic models of phenylketonuria and non-phenylketonuria hyperphenylalaninemia. Anal. Biochem. 280, 242–249 (2000).
Öngür, D., Prescot, A. P., Jensen, J. E., Cohen, B. M. & Renshaw, P. F. Creatine abnormalities in schizophrenia and bipolar disorder. Psychiatry Res. Neuroimaging 172, 44–48 (2009).
Meltzer, H. Y. Serum creatine phosphokinase in schizophrenia. Am. J. Psychiatry 133, 192–197 (1976).
Manor, I. et al. Recurrence pattern of serum creatine phosphokinase levels in repeated acute psychosis. Biol. Psychiatry 43, 288–292 (1998).
Yu, B. et al. The Consortium of Metabolomics Studies (COMETS): Metabolomics in 47 Prospective Cohort Studies. Am. J. Epidemiol. 188, 991–1012 (2019).
Way, G. P. & Greene, C. S. Extracting a biologically relevant latent space from cancer transcriptomes with variational autoencoders. In Pacific Symposium on Biocomputing 0, 80–95 (World Scientific Publishing Co. Pte Ltd, 2018).
Kang, H. M. et al. Multiplexed droplet single-cell RNA-sequencing using natural genetic variation. Nat. Biotechnol. 36, 89–94 (2018).
Hagai, T. et al. Gene expression variability across cells and species shapes innate immunity. Nature 563, 197–202 (2018).
Zheng, G. X. Y. et al. Massively parallel digital transcriptional profiling of single cells. Nat. Commun. 8, 14049 (2017).
Deng, J. et al. ImageNet: A large-scale hierarchical image database. in 248–255 (Institute of Electrical and Electronics Engineers (IEEE), 2010). https://doi.org/10.1109/cvpr.2009.5206848
Lin, T. Y. et al. Microsoft COCO: Common objects in context. in Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics) 8693 LNCS, 740–755 (Springer Verlag, 2014).
Krizhevsky, A. Learning Multiple Layers of Features from Tiny Images. Technical Report, University of Toronto (2009). https://www.cs.toronto.edu/~kriz/learning-features-2009-TR.pdf
Bowman, S. R., Angeli, G., Potts, C. & Manning, C. D. A large annotated corpus for learning natural language inference. Conf. Proc. - EMNLP 2015 Conf. Empir. Methods Nat. Lang. Process. 632–642 (2015).
Nightingale Health and UK Biobank announces major initiative to analyse half a million blood samples to facilitate global medical research. (2018). https://www.ukbiobank.ac.uk/learn-more-about-uk-biobank/news/nightingale-health-and-uk-biobank-announces-major-initiative-to-analyse-half-a-million-blood-samples-to-facilitate-global-medical-research. Accessed 14 Jan 2021.
Mook-Kanamori, D. O. et al. 1,5-Anhydroglucitol in Saliva Is a Noninvasive Marker of Short-Term Glycemic Control. J. Clin. Endocrinol. Metab. 99, E479–E483 (2014).
Hammoudeh, S. et al. The prevalence of metabolic syndrome in patients receiving antipsychotics in Qatar: A cross sectional comparative study. BMC Psychiatry 18, 81 (2018).
Evans, A. M., DeHaven, C. D., Barrett, T., Mitchell, M. & Milgram, E. Integrated, nontargeted ultrahigh performance liquid chromatography/ electrospray ionization tandem mass spectrometry platform for the identification and relative quantification of the small-molecule complement of biological systems. Anal. Chem. 81, 6656–6667 (2009).
Yu, Z. et al. Differences between human plasma and serum metabolite profiles. PLoS One 6, e21230 (2011).
Do, K. T. et al. Characterization of missing values in untargeted MS-based metabolomics data and evaluation of missing data handling strategies. Metabolomics 14, 128 (2018).
Glorot, X. & Bengio, Y. Understanding the difficulty of training deep feedforward neural networks. J. Mach. Learn. Res. - Proc. Track 9, 249–256 (2010).
Maas, A. L., Hannun, A. Y. & Ng, A. Y. Rectifier Nonlinearities Improve Neural Network Acoustic Models. Proceedings of the 30 th International Conference on Machine Learning, Atlanta, Georgia, USA (2013).
Pedregosa, F. et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 12, 2825–2830 (2011).
Gomari, D. P., Schweickart, A. & Krumsiek, J. krumsieklab/mtVAE: Final version for publication. https://doi.org/10.5281/ZENODO.6533078 (2022).
Acknowledgements
The construction of the deep learning models was supported by Google Cloud. This work was also partially supported by the National Cancer Institute of the National Institutes of Health under the awards U10CA180820, UG1CA189859; and by the National Institute of Aging of the National Institutes of Health under award 1U19AG063744. TwinsUK is funded by the Wellcome Trust, Medical Research Council, European Union, the National Institute for Health Research (NIHR)-funded BioResource, Research Facility and Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust in partnership with King’s College London.
Author information
Authors and Affiliations
Contributions
L.C., E.P., and H.F. provided the acute myeloid leukemia data. H.A. provided the schizophrenia data. K.S. provided the QMDiab data. D.P.G. and J.K. conceived of and designed the research study. D.P.G. and A.S. performed model training, experiments, and analyzed all data and results. A.S. processed the datasets. D.P.G., A.S., and J.K. wrote the manuscript. All authors gave final approval to publish.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Biology thanks the anonymous reviewers for their contribution to the peer review of this work. Primary Handling Editor: Luke R. Grinham and Jaume Bacardit.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gomari, D.P., Schweickart, A., Cerchietti, L. et al. Variational autoencoders learn transferrable representations of metabolomics data. Commun Biol 5, 645 (2022). https://doi.org/10.1038/s42003-022-03579-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s42003-022-03579-3
This article is cited by
-
Immune, metabolic landscapes of prognostic signatures for lung adenocarcinoma based on a novel deep learning framework
Scientific Reports (2024)
-
Statistical methods and resources for biomarker discovery using metabolomics
BMC Bioinformatics (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
