
Does Portal Hypertension Increase the Risk of Helicobacter pylori Infection and Pre-Malignant Gastric Lesions?

Abstract
:1. Introduction
2. Methods
2.1. Study Design, Inclusion and Exclusion Criteria
2.2. Data Collection

2.3. Transient Elastography Examination (LSM and SSM)
2.4. Esophago-Gastroduodenoscopies (EGD)
2.5. Helicobacter Pylori Detection and Pre-Malignant Gastric Lesions Diagnosis
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Study Population
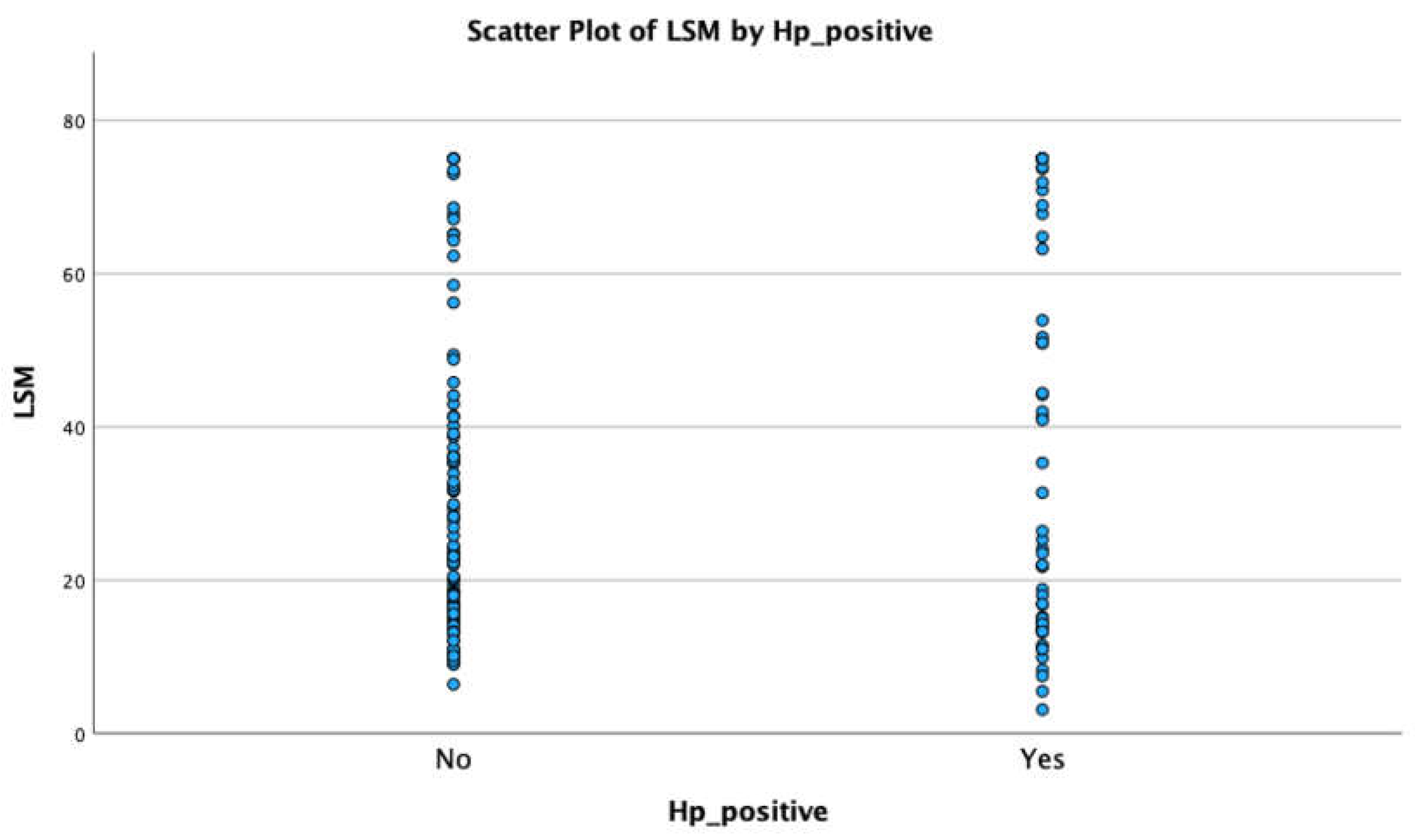
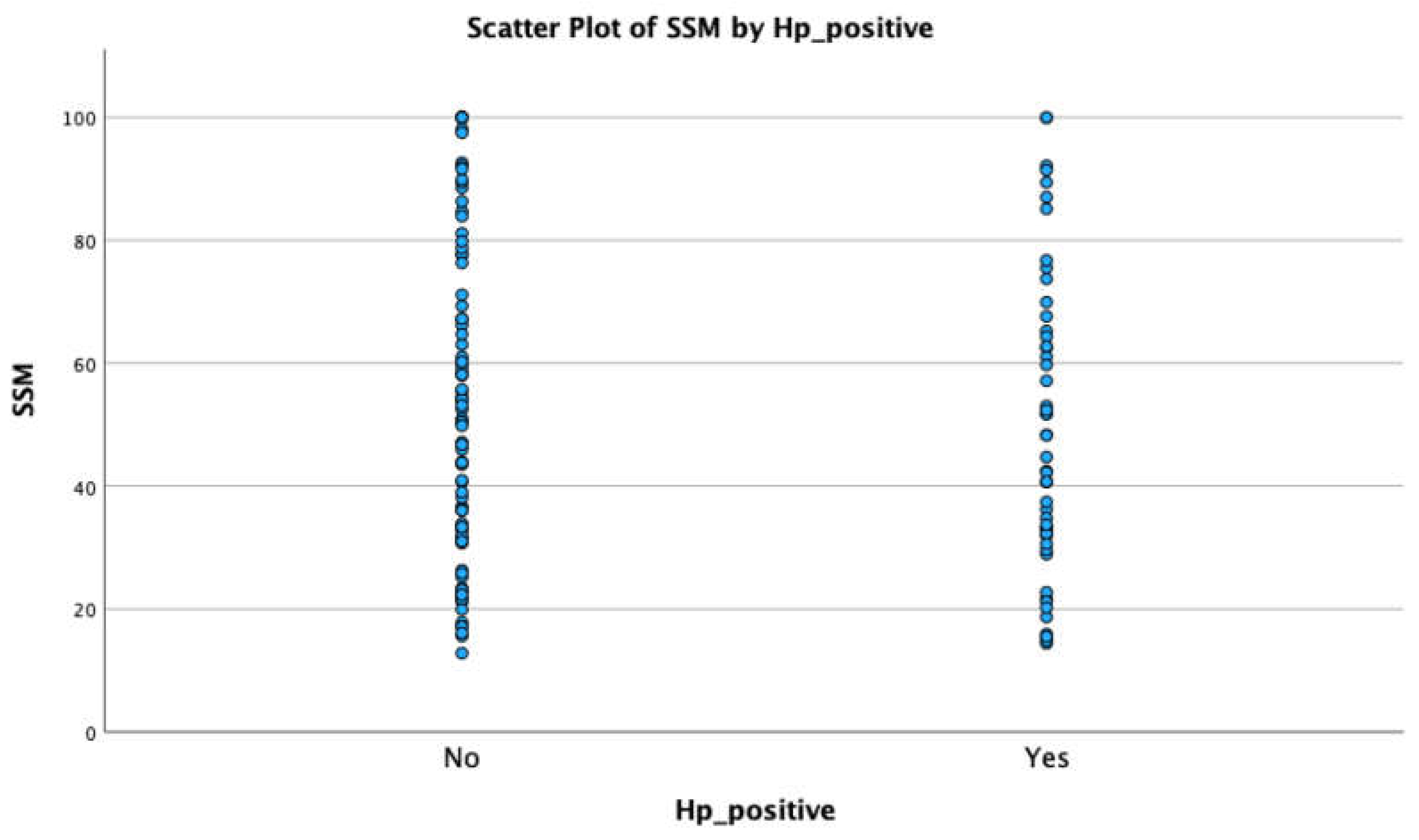
3.2. LSM and SSM
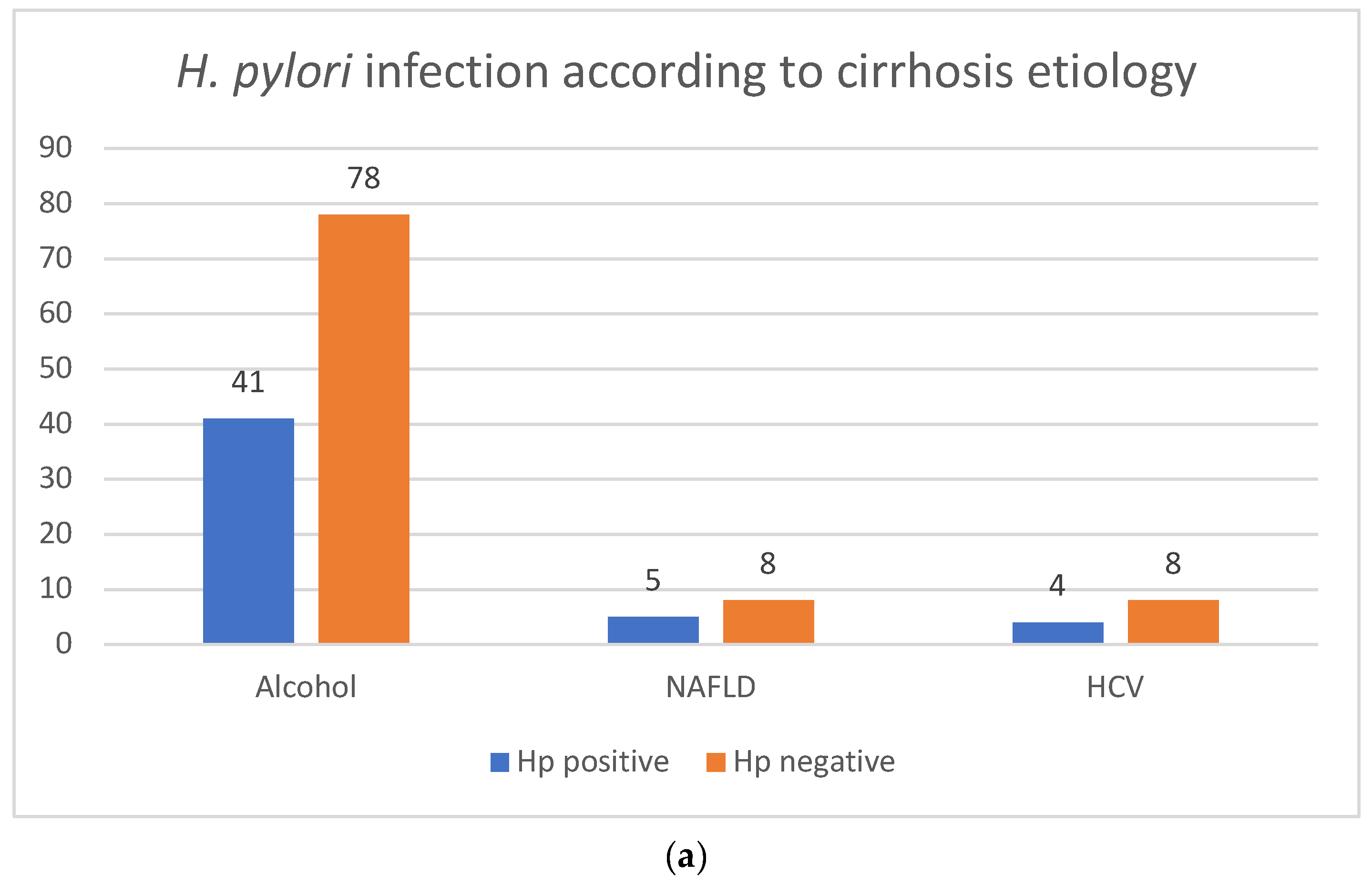
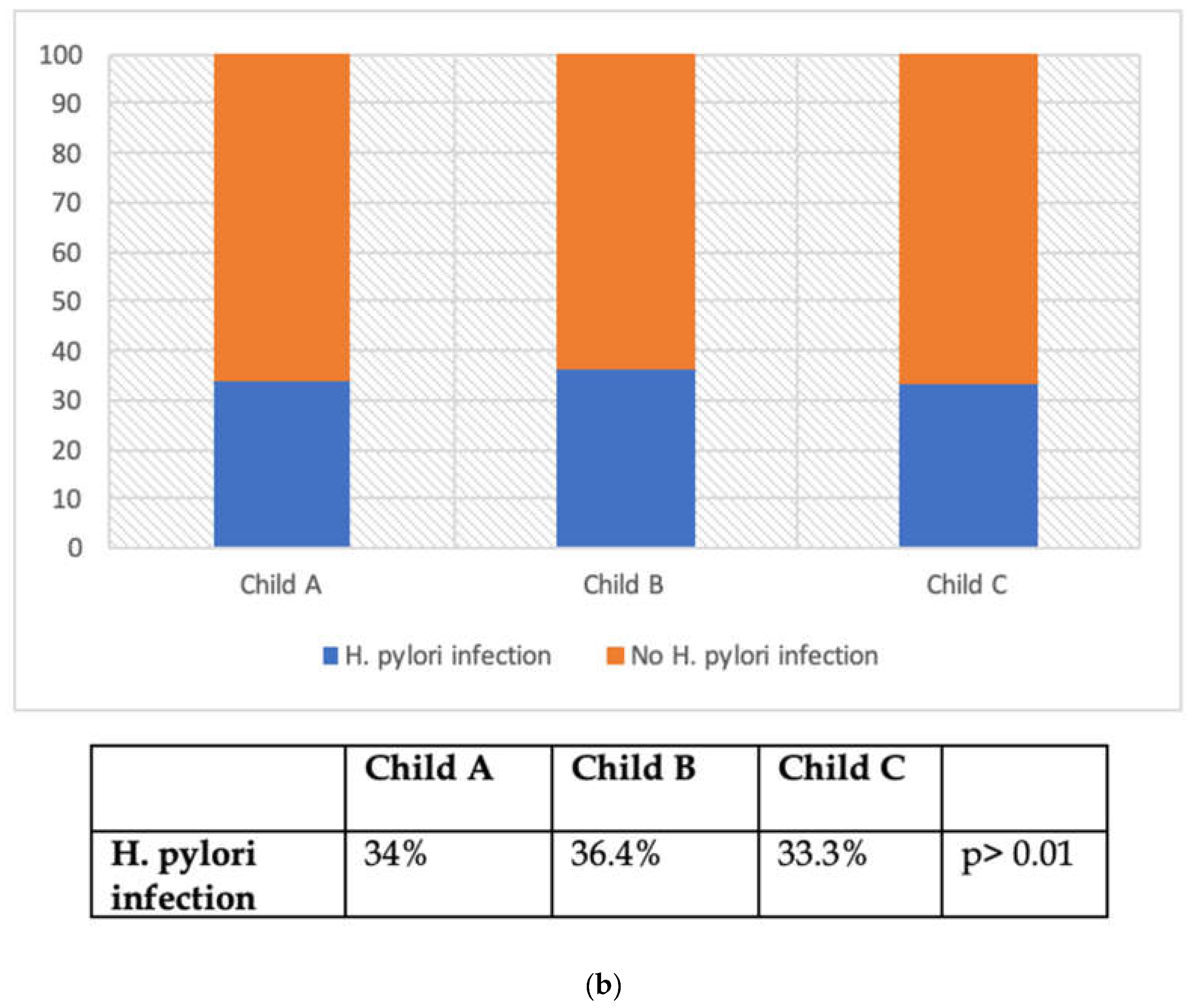
3.3. H. pylori Infection
3.4. Endoscopic and Histologic Findings




4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AFP | Alpha-fetoprotein |
| AIH | Autoimmune hepatitis |
| ALP | Alkaline phosphatase |
| ALT | Alanine aminotransferase |
| AST | Aspartate aminotransferase |
| CSPH | Clinically significant portal hypertension |
| EGD | Esophago-gastroduodenoscopy |
| GGT | Gamma-glutamyl transferase |
| HBV | Hepatitis B virus |
| HCV | Hepatitis C virus |
| H. pylori | Helibobacter pylori |
| HVPG | Hepatic venous pressure gradient |
| IL 1B | Interleucin 1B |
| IL 8 | Interleucin 8 |
| IL 10 | Interleucin 10 |
| INR | International normalized ratio |
| IQR | Interquartile range |
| LSM | Liver stiffness measurement |
| MALT | Mucosa-associated lymphoid tissue |
| MRI | Magnetic resonance imaging |
| NAFLD | Non-alcoholic liver disease |
| OLGA | Operative Link on Gastritis Assessment |
| OLGIM | operative link on intestinal metaplasia assessment |
| PHG | Portal hypertension gastropathy |
| PLT | Platelet |
| PBC | Primary biliary cholangitis |
| SSM | Spleen stiffness measurement |
| VEGF | Vascular endothelial growth factor |
References
- Zhou, W.C.; Zhang, Q.B.; Qiao, L. Pathogenesis of liver cirrhosis. World J. Gastroenterol. 2014, 20, 7312–7324. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Cirrhosis Collaborators. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.B.; Chen, M.K. Epidemiology of liver cirrhosis and associated complications: Current knowledge and future directions. World J. Gastroenterol. 2022, 28, 5910–5930. [Google Scholar] [CrossRef] [PubMed]
- Reiberger, T. The Value of Liver and Spleen Stiffness for Evaluation of Portal Hypertension in Compensated Cirrhosis. Hepatol. Commun. 2022, 6, 950–964. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Abraldes, J.G.; Berzigotti, A.; Bosch, J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017, 65, 310–335. [Google Scholar] [CrossRef]
- Bosch, J.; Abraldes, J.G.; Berzigotti, A.; Garcia-Pagan, J.C. The clinical use of HVPG measurements in chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.C.; Loong, T.C.; Pang, J.; Wei, J.L.; Wong, V.W. Invasive and non-invasive assessment of portal hypertension. Hepatol. Int. 2018, 12 (Suppl. S1), 44–55. [Google Scholar] [CrossRef]
- Colecchia, A.; Marasco, G.; Taddia, M.; Montrone, L.; Eusebi, L.H.; Mandolesi, D.; Schiumerini, R.; Di Biase, A.R.; Festi, D. Liver and spleen stiffness and other noninvasive methods to assess portal hypertension in cirrhotic patients: A review of the literature. Eur. J. Gastroenterol. Hepatol. 2015, 27, 992–1001. [Google Scholar] [CrossRef]
- Lemoine, M.; Katsahian, S.; Ziol, M.; Nahon, P.; Ganne-Carrie, N.; Kazemi, F.; Grando-Lemaire, V.; Trinchet, J.C.; Beaugrand, M. Liver stiffness measurement as a predictive tool of clinically significant portal hypertension in patients with compensated hepatitis C virus or alcohol-related cirrhosis. Aliment. Pharmacol. Ther. 2008, 28, 1102–1110. [Google Scholar] [CrossRef]
- Vizzutti, F.; Arena, U.; Romanelli, R.G.; Rega, L.; Foschi, M.; Colagrande, S.; Petrarca, A.; Moscarella, S.; Belli, G.; Zignego, A.L.; et al. Liver stiffness measurement predicts severe portal hypertension in patients with HCV-related cirrhosis. Hepatology 2007, 45, 1290–1297. [Google Scholar] [CrossRef]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Baveno, V.I.I.F. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Stefanescu, H.; Grigorescu, M.; Lupsor, M.; Procopet, B.; Maniu, A.; Badea, R. Spleen stiffness measurement using Fibroscan for the noninvasive assessment of esophageal varices in liver cirrhosis patients. J. Gastroenterol. Hepatol. 2011, 26, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Huang, J.; Huang, H.; Liu, S.; Luo, Y. Performance of spleen stiffness measurement in prediction of clinical significant portal hypertension: A meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Stefanescu, H.; Rusu, C.; Lupsor-Platon, M.; Nicoara Farcau, O.; Fischer, P.; Grigoras, C.; Horhat, A.; Stancu, O.; Ardelean, A.; Tantau, M.; et al. Liver Stiffness Assessed by Ultrasound Shear Wave Elastography from General Electric Accurately Predicts Clinically Significant Portal Hypertension in Patients with Advanced Chronic Liver Disease. Ultraschall Med. 2020, 41, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, H.; Katelaris, P. Epidemiology, clinical impacts and current clinical management of Helicobacter pylori infection. Med. J. Aust. 2016, 204, 376–380. [Google Scholar] [CrossRef]
- Waluga, M.; Kukla, M.; Zorniak, M.; Bacik, A.; Kotulski, R. From the stomach to other organs: Helicobacter pylori and the liver. World J. Hepatol. 2015, 7, 2136–2146. [Google Scholar] [CrossRef]
- Kusters, J.G.; van Vliet, A.H.; Kuipers, E.J. Pathogenesis of Helicobacter pylori infection. Clin. Microbiol. Rev. 2006, 19, 449–490. [Google Scholar] [CrossRef]
- Franceschi, F.; Zuccala, G.; Roccarina, D.; Gasbarrini, A. Clinical effects of Helicobacter pylori outside the stomach. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 234–242. [Google Scholar] [CrossRef]
- Licinio, R.; Losurdo, G.; Carparelli, S.; Iannone, A.; Giorgio, F.; Barone, M.; Principi, M.; Ierardi, E.; Di Leo, A. Helicobacter pylori, liver cirrhosis, and portal hypertension: An updated appraisal. Immunopharmacol. Immunotoxicol. 2016, 38, 408–413. [Google Scholar] [CrossRef]
- Serin, E.; Pourbagher, M.A.; Gumurdulu, Y.; Tamer, L.; Ozer, B.; Yilmaz, U. The effect of decrease in serum nitric oxide concentration on portal hemodynamics after Helicobacter pylori treatment: An open-label pilot study. Turk. J. Gastroenterol. 2008, 19, 158–162. [Google Scholar]
- Yakut, M.; Ormeci, N.; Erdal, H.; Keskin, O.; Karayel, Z.; Tutkak, H.; Soykan, I. The association between precancerous gastric lesions and serum pepsinogens, serum gastrin, vascular endothelial growth factor, serum interleukin-1 Beta, serum toll-like receptor-4 levels and Helicobacter pylori Cag A status. Clin. Res. Hepatol. Gastroenterol. 2013, 37, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Jun, Y.K.; Kim, J.W.; Kim, B.G.; Lee, K.L.; Jung, Y.J.; Kim, W.; Park, H.S.; Lee, D.H.; Koh, S.J. Helicobacter pylori infection is not associated with portal hypertension-related gastrointestinal complications: A meta-analysis. PLoS ONE 2022, 17, e0261448. [Google Scholar] [CrossRef]
- Abdel-Hady, H.; Zaki, A.; Badra, G.; Lotfy, M.; Selmi, C.; Giorgini, A.; El-Sayed, M.; Badr, R. Helicobacter pylori infection in hepatic encephalopathy: Relationship to plasma endotoxins and blood ammonia. Hepatol. Res. 2007, 37, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- LeVeen, H.H.; LeVeen, E.G.; LeVeen, R.F. Awakenings to the pathogenicity of urease and the requirement for continuous long term therapy. Biomed. Pharmacother. 1994, 48, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Schutte, K.; Malfertheiner, P. Does H. pylori eradication therapy benefit patients with hepatic encephalopathy?: Systematic review. J. Clin. Gastroenterol. 2014, 48, 491–499. [Google Scholar] [CrossRef]
- Zullo, A.; Hassan, C.; Morini, S. Helicobacter pylori infection in patients with liver cirrhosis: Facts and fictions. Dig. Liver Dis. 2003, 35, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Pogorzelska, J.; Lapinska, M.; Kalinowska, A.; Lapinski, T.W.; Flisiak, R. Helicobacter pylori infection among patients with liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1161–1165. [Google Scholar] [CrossRef]
- Castera, L.; Forns, X.; Alberti, A. Non-invasive evaluation of liver fibrosis using transient elastography. J. Hepatol. 2008, 48, 835–847. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitis. J. Hepatol. 2017, 67, 145–172. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Wilson’s disease. J. Hepatol. 2012, 56, 671–685. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines for HFE hemochromatosis. J. Hepatol. 2010, 53, 3–22. [Google Scholar] [CrossRef]
- Greene, C.M.; Marciniak, S.J.; Teckman, J.; Ferrarotti, I.; Brantly, M.L.; Lomas, D.A.; Stoller, J.K.; McElvaney, N.G. α1-Antitrypsin deficiency. Nat. Rev. Dis. Primers 2016, 2, 16051. [Google Scholar] [CrossRef]
- McCormack, T.T.; Sims, J.; Eyre-Brook, I.; Kennedy, H.; Goepel, J.; Johnson, A.G.; Triger, D.R. Gastric lesions in portal hypertension: Inflammatory gastritis or congestive gastropathy? Gut 1985, 26, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Libanio, D.; Marcos-Pinto, R.; Areia, M.; Leja, M.; Esposito, G.; Garrido, M.; Kikuste, I.; Megraud, F.; Matysiak-Budnik, T.; et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy 2019, 51, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Price, A.B. The Sydney System: Histological division. J. Gastroenterol. Hepatol. 1991, 6, 209–222. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.H.; Potthoff, A.; Ledig, S.; Cornberg, M.; Jandl, O.; Manns, M.P.; Kubicka, S.; Flemming, P.; Athmann, C.; Beil, W.; et al. Effect of H. pylori on the expression of TRAIL, FasL and their receptor subtypes in human gastric epithelial cells and their role in apoptosis. Helicobacter 2004, 9, 371–386. [Google Scholar] [CrossRef]
- Feng, H.; Zhou, X.; Zhang, G. Association between cirrhosis and Helicobacter pylori infection: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2014, 26, 1309–1319. [Google Scholar] [CrossRef]
- Sanchez-Mete, L.; Zullo, A.; Hassan, C.; Rinaldi, V.; Magno, M.S.; Festuccia, F.; Morini, S.; Attili, A.F. Helicobacter pylori diagnosis in patients with liver cirrhosis. Dig. Liver Dis. 2003, 35, 566–570. [Google Scholar] [CrossRef]
- Nurgalieva, Z.Z.; Opekun, A.R.; Graham, D.Y. Problem of distinguishing false-positive tests from acute or transient Helicobacter pylori infections. Helicobacter 2006, 11, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Calvet, X.; Navarro, M.; Gil, M.; Mas, P.; Rivero, E.; Sanfeliu, I.; Brullet, E.; Campo, R.; Dalmau, B.; Lafont, A. Seroprevalence and epidemiology of Helicobacter pylori infection in patients with cirrhosis. J. Hepatol. 1997, 26, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.T.; Wang, T.F.; Chan, C.C.; Lee, F.Y.; Chang, F.Y.; Lin, H.C.; Hou, M.C.; Lu, R.H.; Chu, C.J.; Wang, S.S.; et al. Role of chronic Helicobacter pylori infection in hyperdynamic circulation of cirrhotic patients. Hepatogastroenterology 2002, 49, 208–212. [Google Scholar] [PubMed]
- Yu, Y.Y.; Tong, Y.L.; Wu, L.Y.; Yu, X.Y. Helicobacter pylori infection eradication for nonalcoholic fatty liver disease: A randomized controlled trial. Sci. Rep. 2022, 12, 19530. [Google Scholar] [CrossRef] [PubMed]
- Abo-Amer, Y.E.; Sabal, A.; Ahmed, R.; Hasan, N.F.E.; Refaie, R.; Mostafa, S.M.; Mohamed, A.A.; Khalil, M.; Elagawy, W.; Abd-Elsalam, S. Relationship between Helicobacter pylori Infection and Nonalcoholic Fatty Liver Disease (NAFLD) in a Developing Country: A Cross-Sectional Study. Diabetes Metab. Syndr. Obes. 2020, 13, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Maharshi, V.; Gupta, P.; Kumar, V.L.; Upadhyay, A.D.; Das, P.; Yadav, R.; Nayak, B.; Kumar, R.; Shalimar. Effect of Helicobacter pylori-eradication therapy on hepatic steatosis in patients with non-alcoholic fatty liver disease: A randomized-controlled pilot study. Gastroenterol. Rep. 2020, 8, 104–110. [Google Scholar] [CrossRef]
- Alarfaj, S.J.; Abdallah Mostafa, S.; Abdelsalam, R.A.; Negm, W.A.; El-Masry, T.A.; Hussein, I.A.; El Nakib, A.M. Helicobacter pylori Infection in Cirrhotic Patients With Portal Hypertensive Gastropathy: A New Enigma? Front. Med. 2022, 9, 902255. [Google Scholar] [CrossRef] [PubMed]
- Hammad, O.M.; Abu-Seif, M.A.; Ashour, M.; Hifnawy, T. Correlation of portal hypertensive gastropathy with Helicobacter pylori infection, liver dysfunction, hypersplenism and oesophageal varices. Med. J. Cairo Univ. 2009, 77, 597–601. [Google Scholar]
- Hu, J.K.; Li, X.M.; Gu, B.H.; Zhang, F.; Li, Y.M.; Chen, H. Helicobacter pylori and portal hypertensive gastropathy. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 578–580. [Google Scholar] [CrossRef]
- Sipponen, P.; Graham, D.Y. Importance of atrophic gastritis in diagnostics and prevention of gastric cancer: Application of plasma biomarkers. Scand. J. Gastroenterol. 2007, 42, 2–10. [Google Scholar] [CrossRef]
- Roman, L.D.; Lukyanchuk, R.; Sablin, O.A.; Araslanova, E.I.; Eklund, C.; Hendolin, P.; Paloheimo, L.; Syrjanen, K. Prevalence of H. pylori Infection and Atrophic Gastritis in a Population-based Screening with Serum Biomarker Panel (GastroPanel(R)) in St. Petersburg. Anticancer Res. 2016, 36, 4129–4138. [Google Scholar] [PubMed]
- Tepes, B.; Seruga, M.; Vujasinovic, M.; Urlep, D.; Ljepovic, L.; Brglez, J.N.; Forte, A.; Anita Kek, L.; Skvarc, M. Premalignant Gastric Lesions in Patients Included in National Colorectal Cancer Screening. Radiol. Oncol. 2018, 52, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Jeng, K.S.; Chang, C.F.; Sheen, I.S.; Jeng, C.J.; Wang, C.H. Upper Gastrointestinal Cancer and Liver Cirrhosis. Cancers 2022, 14, 2269. [Google Scholar] [CrossRef] [PubMed]
- Zullo, A.; Romiti, A.; Tomao, S.; Hassan, C.; Rinaldi, V.; Giustini, M.; Morini, S.; Taggi, F. Gastric cancer prevalence in patients with liver cirrhosis. Eur. J. Cancer Prev. 2003, 12, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Zullo, A.; Romiti, A.; Rinaldi, V.; Vecchione, A.; Hassan, C.; Winn, S.; Tomao, S.; Attili, A.F. Gastric epithelial cell proliferation in patients with liver cirrhosis. Dig. Dis. Sci. 2001, 46, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Vallee, B.L.; Falchuk, K.H. The biochemical basis of zinc physiology. Physiol. Rev. 1993, 73, 79–118. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 155 | |
|---|---|
| Mean age (SD) | 64.1 years (±8.8) |
| Male sex | 126 (81.3%) |
| Cirrhosis diagnosis: LSM Histological | 114 (73.5%) 41 (26.5%) |
| Cirrhosis etiology: Alcohol NAFLD HCV Alcohol + HCV HBV Hemochromatosis Auto-immune hepatitis Drug-induced liver injury Primary biliary cholangitis PBC Alcohol + HBV | 113 (72.9%) 13 (8.5%) 12 (7.7%) 6 (3.9%) 2 (1.3%) 2 (1.3%) 2 (1.3%) 2 (1.3%) 1 (0.6%) 1 (0.6%) 1 (0.6%) |
| n = 155 | |
|---|---|
| LSM (kPa) | 24.4 [3.1–75.0] |
| IQR (%) | 16% [0.0–30.0] |
| CAP (dB/m) | 253.0 [100.0–394.0] |
| IQR (dB/m) | IQR 28.0 [0–145.0] |
| SSM (kPa) | 49.1 [12.8–100] |
| IQR (kPa) | 6.3 [0–39.0] |
| (a) | |
|---|---|
| Stomach Fundus and body Erythema Erosions Atrophy Metaplasia Portal hypertension gastropathy (mild/severe) Antrum and incisura Erythema Erosions Ulcers Atrophy Metaplasia GAVE | 20 (12.9%) 4 (2.6%) 7 (4.5%) 3 (1.9%) 51–45/6 (32.9%–29.0/3.9%) 106 68.4%) 29 (18.7%) 14 (9.0%) 3 (1.9%) 11 (7.1%) 2 (1.3%) |
| (b) | |
| Stomach Atrophy Corpus and fundus Antrum and incisura OLGA 1 OLGA 2 OLGA 3 OLGA 4 Metaplasia Corpus and fundus Antrum and incisura OLGIM 1 OLGIM 2 OLGIM 3 OLGIM 4 | 23 (14.8%) 41 (26.5%) 32 (58.2%) 18 (32.7%) 4 (7.2%) 1 (1.8%) 24 (15.6%) 52 (33.5%) 38 (63.3%) 16 (26.7%) 4 (6.7%) 2 (3.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaspar, R.; Cardoso, P.; Ribeiro, T.; Silva, M.; Macedo, G. Does Portal Hypertension Increase the Risk of Helicobacter pylori Infection and Pre-Malignant Gastric Lesions? J. Clin. Med. 2024, 13, 1768. https://doi.org/10.3390/jcm13061768
Gaspar R, Cardoso P, Ribeiro T, Silva M, Macedo G. Does Portal Hypertension Increase the Risk of Helicobacter pylori Infection and Pre-Malignant Gastric Lesions? Journal of Clinical Medicine. 2024; 13(6):1768. https://doi.org/10.3390/jcm13061768
Chicago/Turabian StyleGaspar, Rui, Pedro Cardoso, Tiago Ribeiro, Marco Silva, and Guilherme Macedo. 2024. "Does Portal Hypertension Increase the Risk of Helicobacter pylori Infection and Pre-Malignant Gastric Lesions?" Journal of Clinical Medicine 13, no. 6: 1768. https://doi.org/10.3390/jcm13061768