
Concordance of LDL-C Estimating Equations with Direct Enzymatic Measurement in Diabetic and Prediabetic Subjects
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Biochemical Analyses
2.3. Lipid Estimations
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
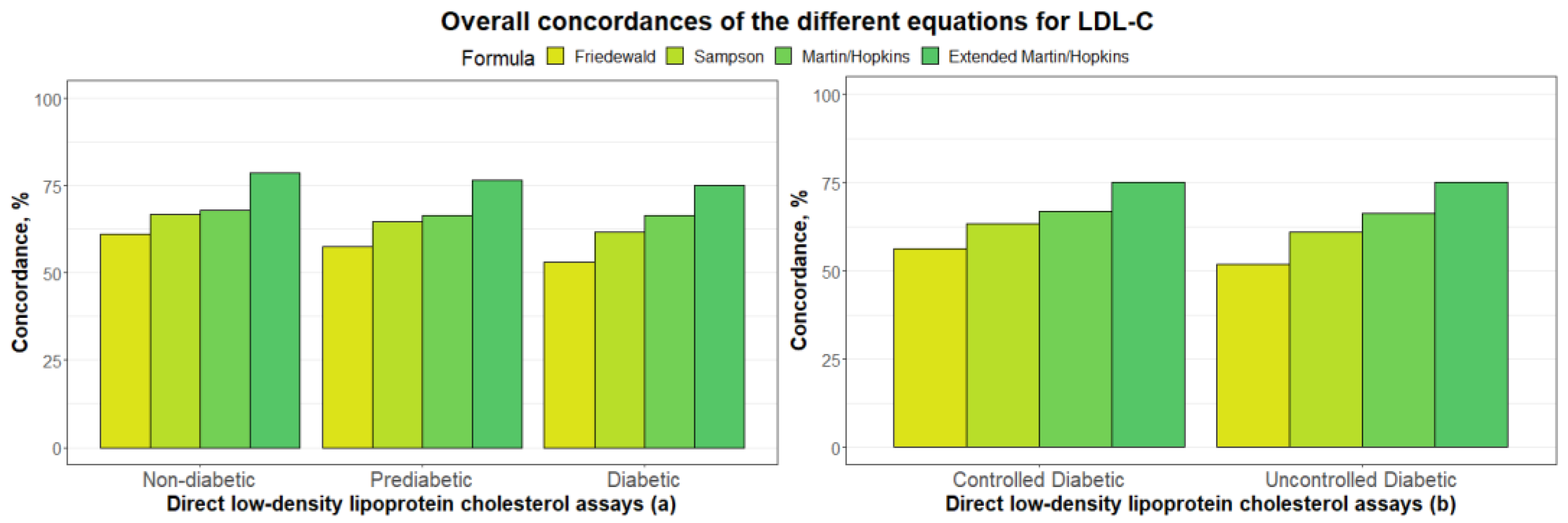
3.2. Overall Concordances of the Various LDL-C Estimating Equations
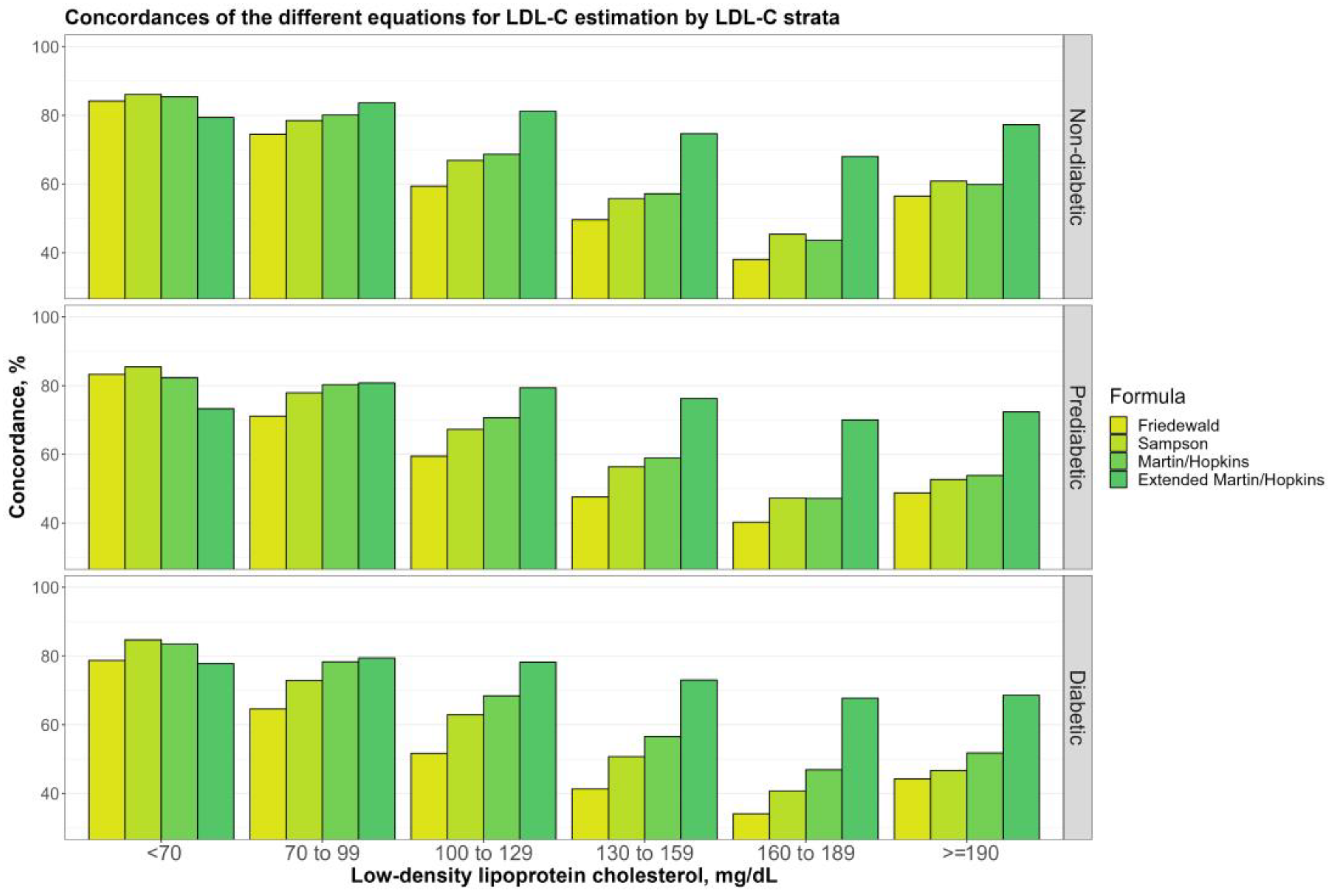
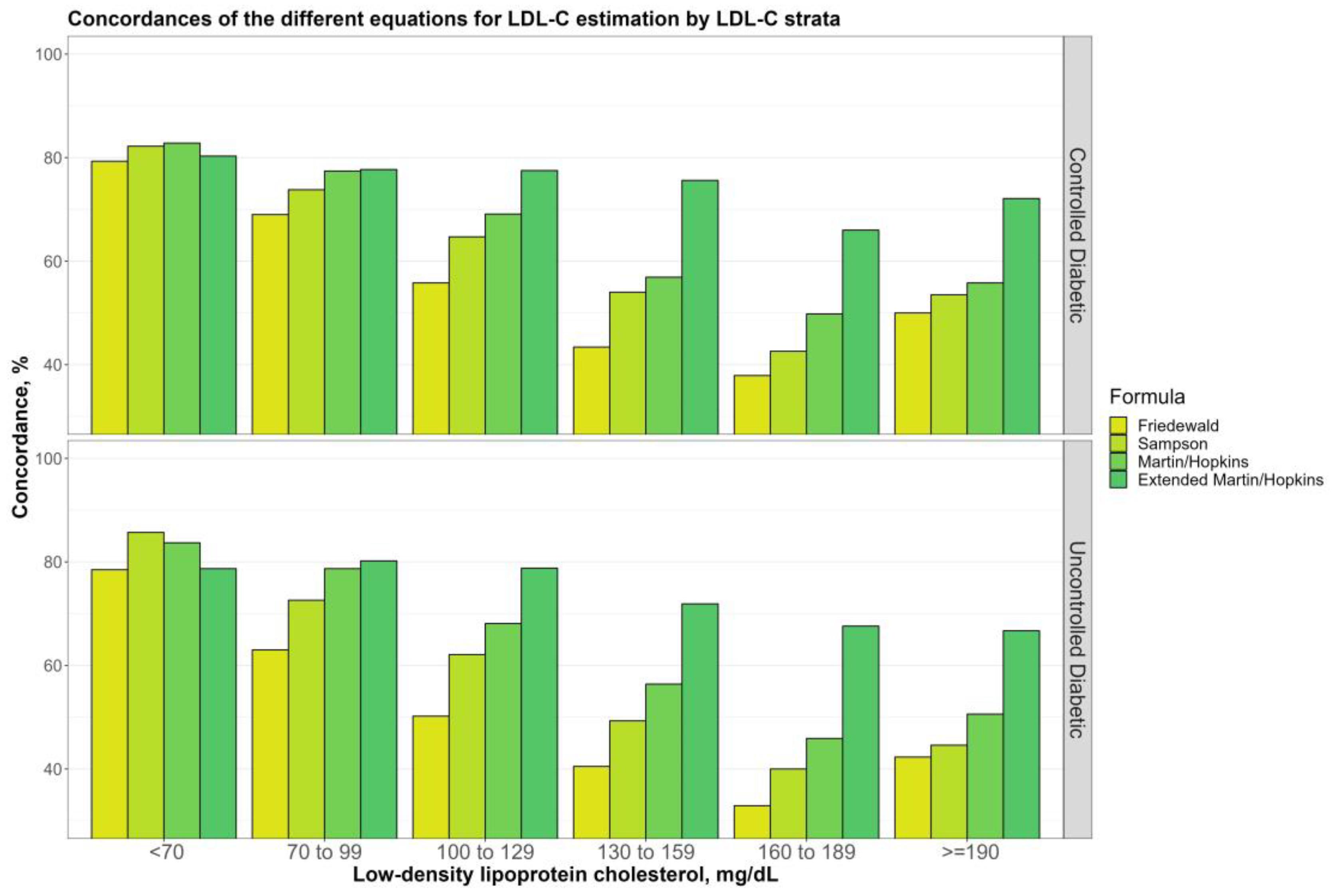
3.3. Overall Concordances of the Various LDL-C Estimating Equations by LDL-C Sublevels
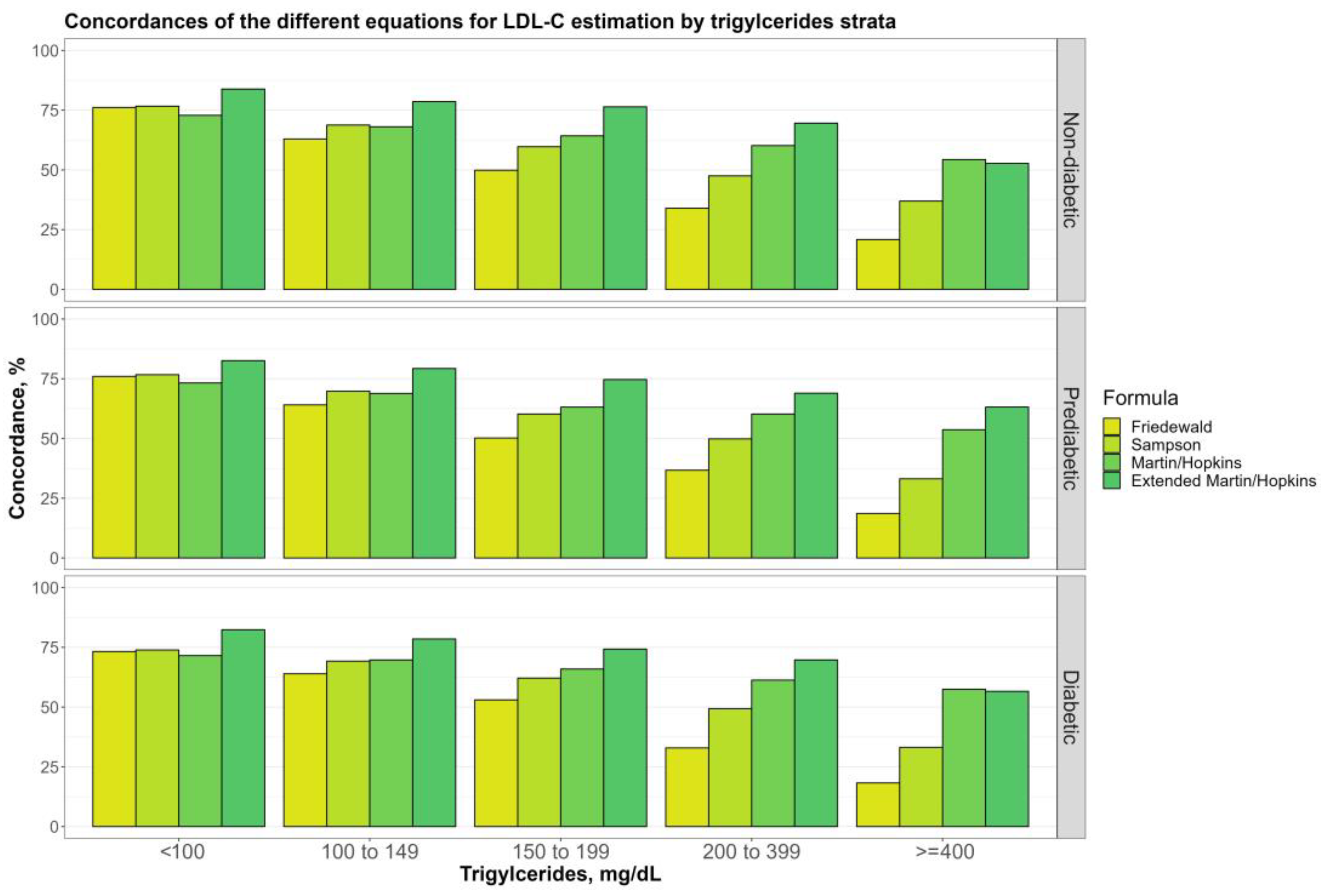
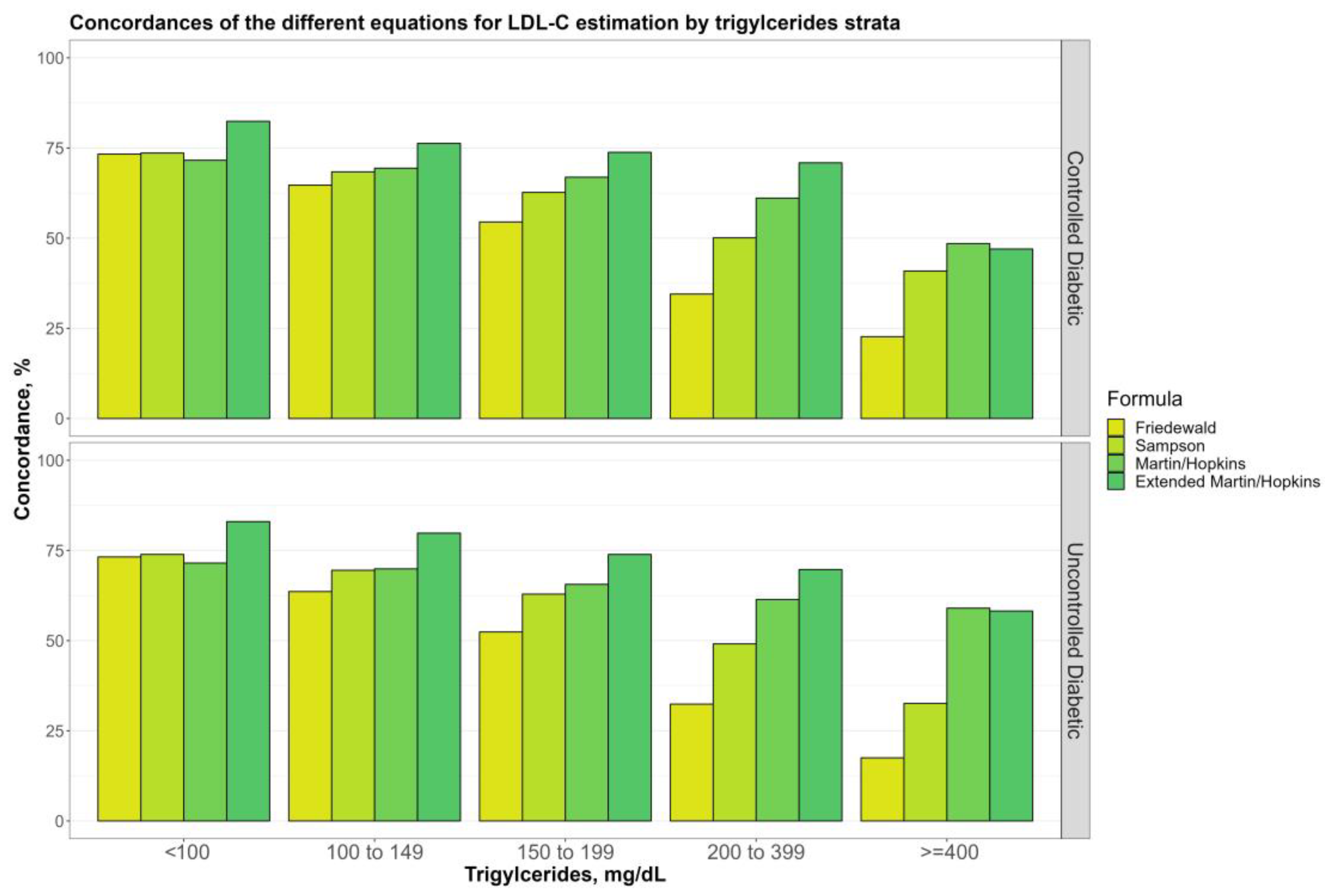
3.4. Overall Concordances of the Various LDL-C Estimating Equations by TG Sublevels
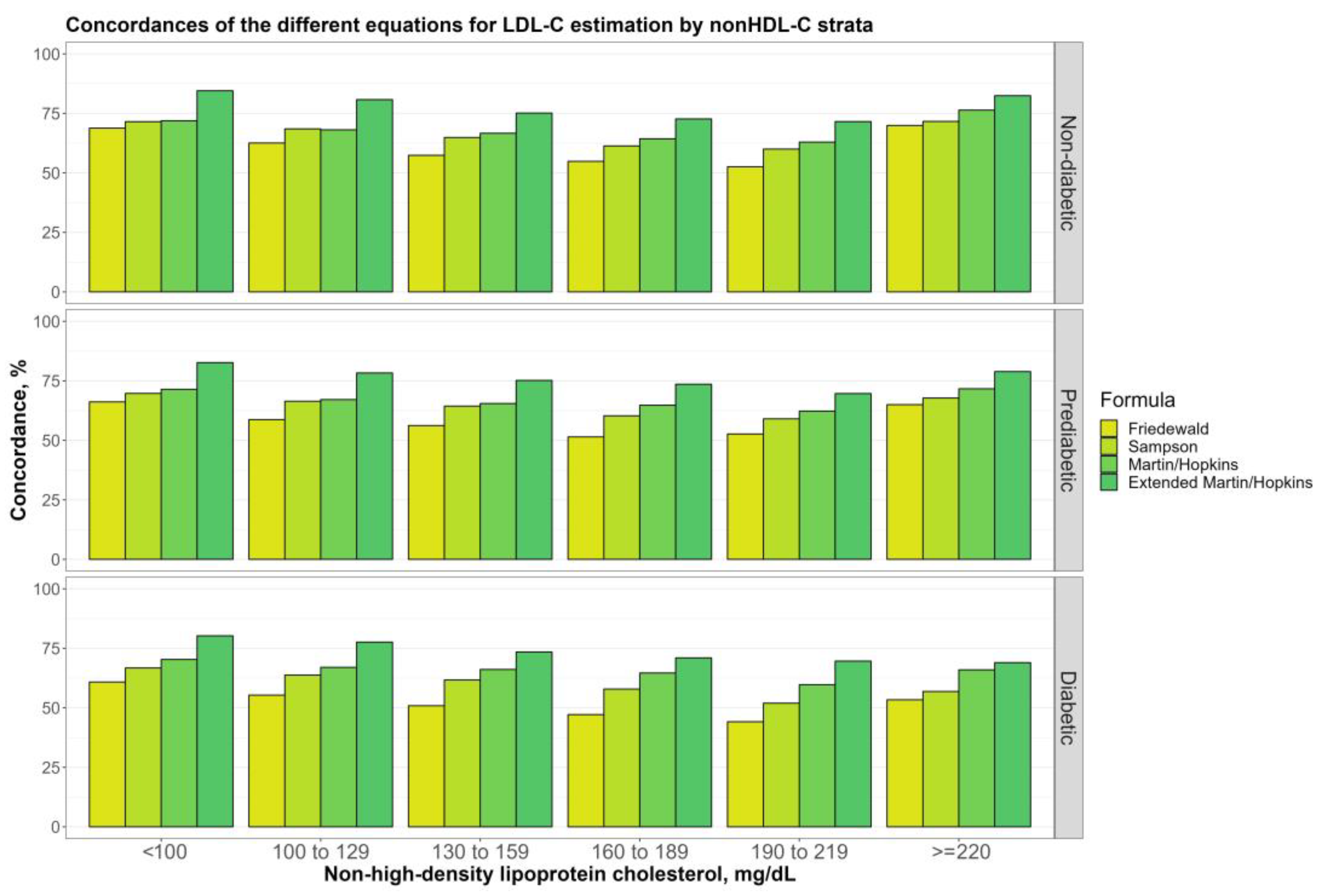
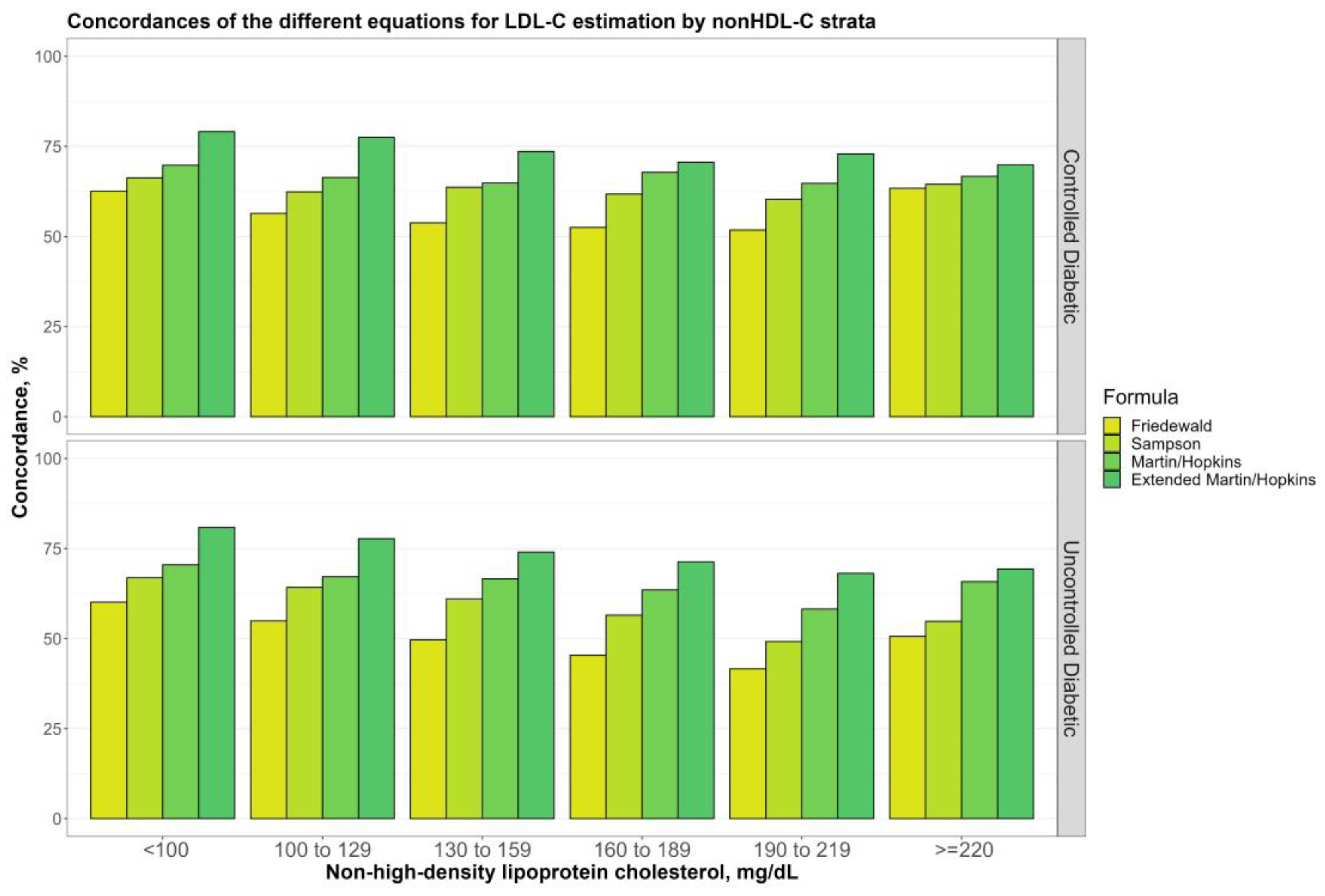
3.5. Overall Concordances of the Various LDL-C Estimating Equations by Non-HDL-C Sublevels
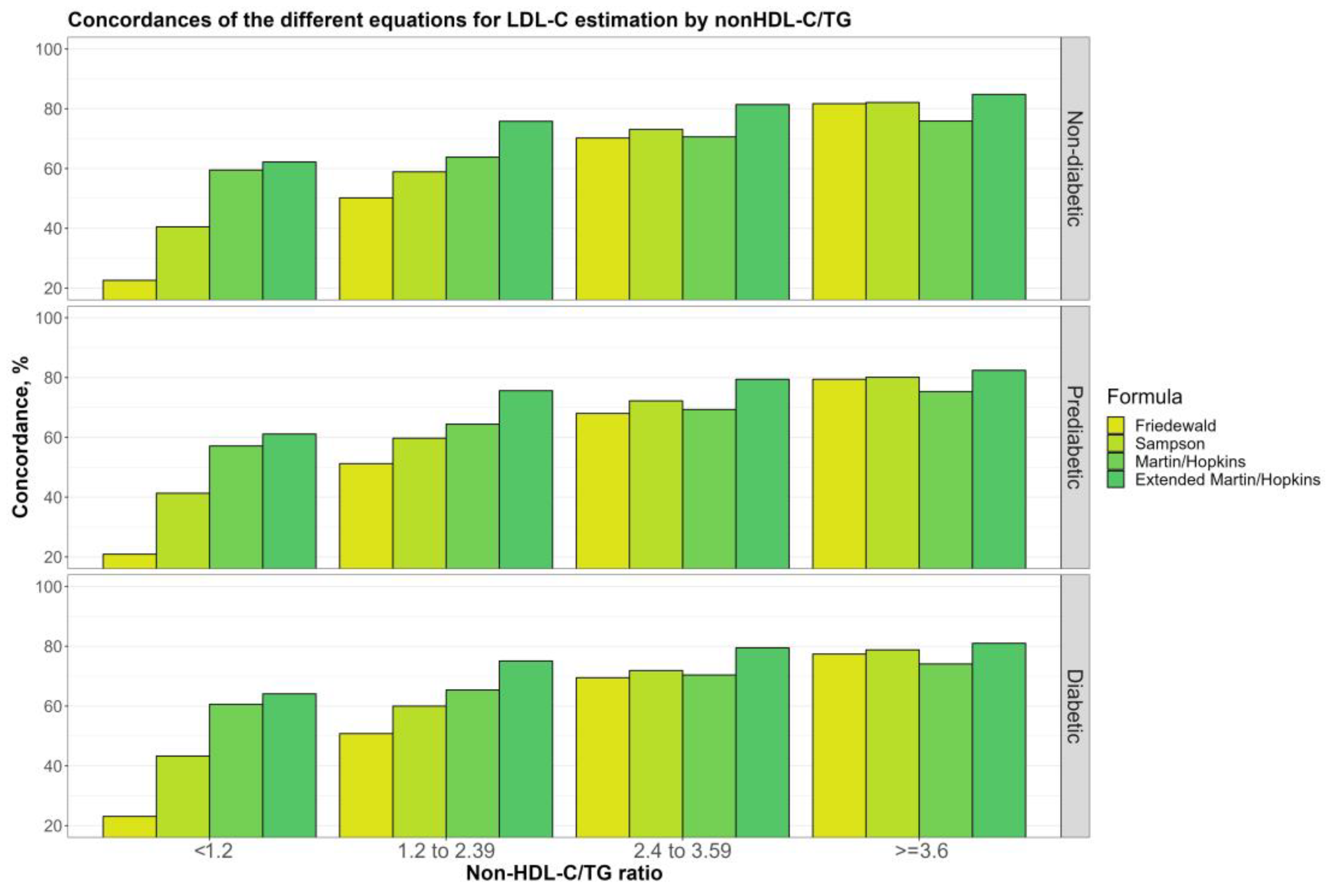
3.6. Overall Concordances of the Various LDL-C Estimating Equations by Non-HDL-C/TG Sublevels
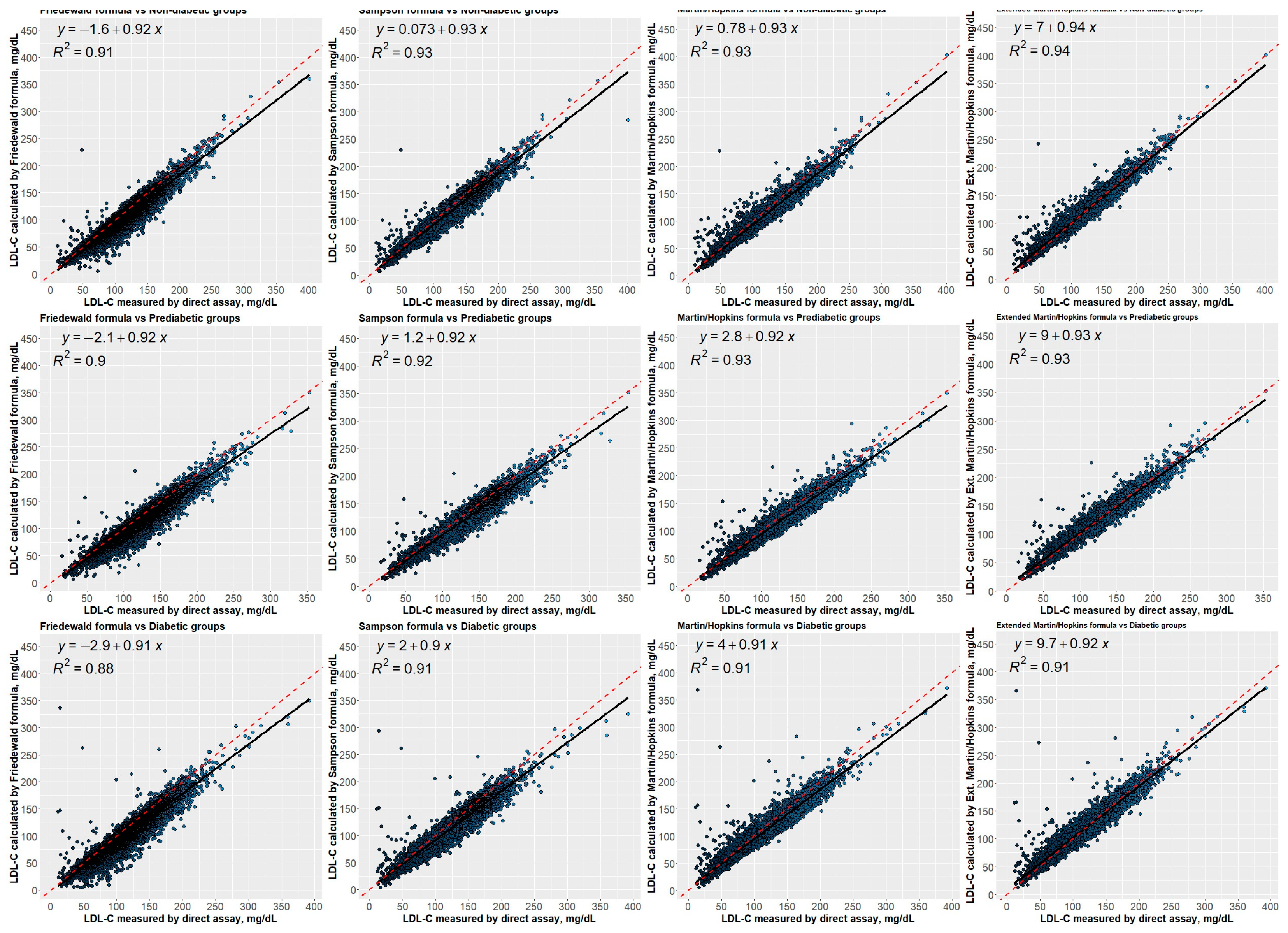
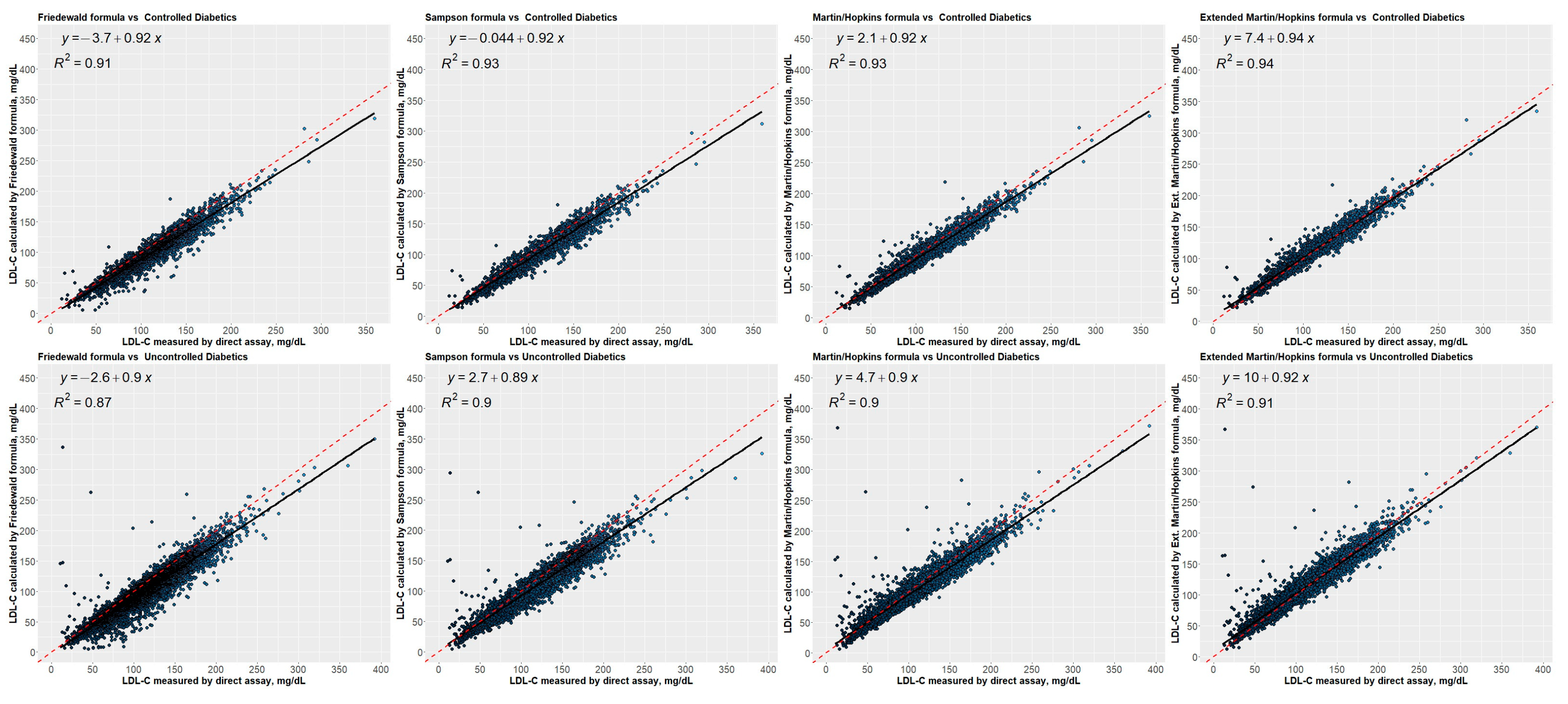
3.7. Correlation between Estimated LDL-C Levels Using Different Equations and Directly Measured LDL-C Levels
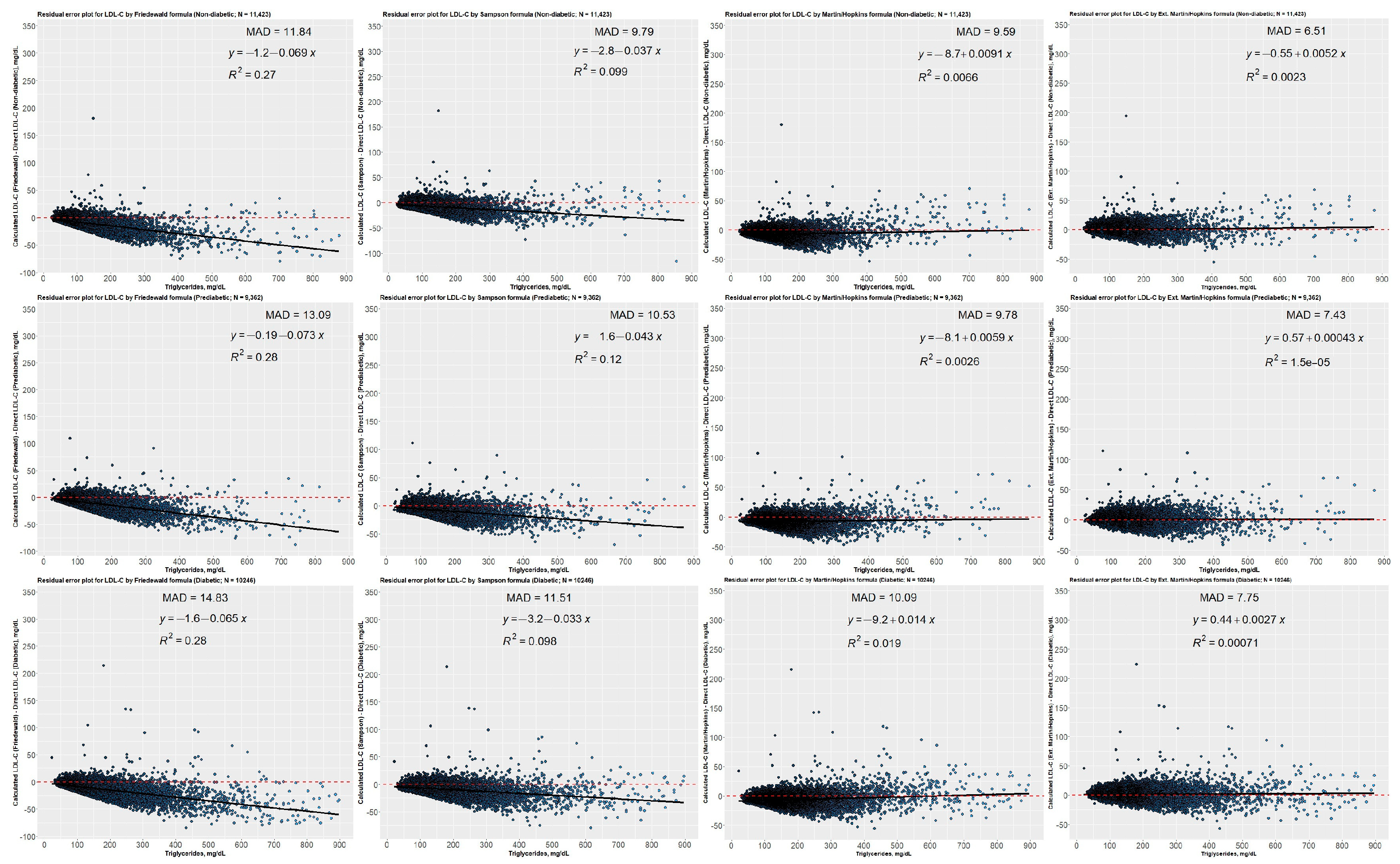
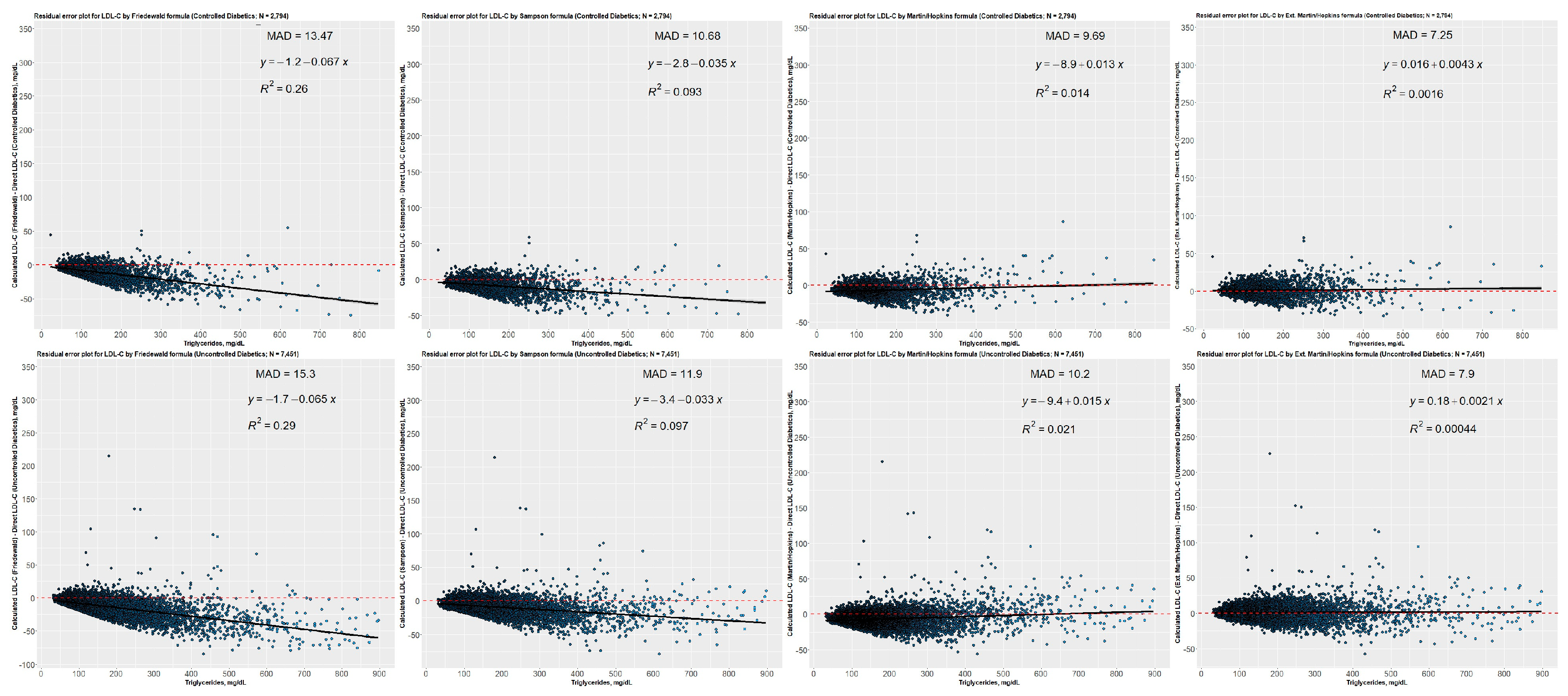
3.8. Residual Error Plots for LDL-C Concentrations Estimated by Different Equations concerning Direct Assay
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. S1), S15–S33. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, Regional and Country-Level Diabetes Prevalence Estimates for 2021 and Projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.P. Effects of Combination Lipid Therapy in Type 2 Diabetes Mellitus. Yearb. Endocrinol. 2010, 2010, 50–52. [Google Scholar] [CrossRef]
- Forbes, J.M.; Cooper, M.E. Mechanisms of Diabetic Complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45 (Suppl. S1), S144–S174. [Google Scholar] [CrossRef] [PubMed]
- Feingold, K.; Siperstein, M.D. Diabetic Vascular Disease. Adv. Intern. Med. 1986, 31, 309–340. [Google Scholar]
- Regensteiner, J.G.; Golden, S.; Anton, B.; Barrett-Connor, E.; Chang, A.Y.; Chyun, D.; Fox, C.S.; Huebschmann, A.G.; Kim, C.; Mehta, N.; et al. Sex Differences in the Cardiovascular Consequences of Diabetes Mellitus a Scientific Statement from the American Heart Association. Circulation 2015, 132, 2424–2447. [Google Scholar] [CrossRef]
- Fox, C.S.; Golden, S.H.; Anderson, C.; Bray, G.A.; Burke, L.E.; De Boer, I.H.; Deedwania, P.; Eckel, R.H.; Ershow, A.G.; Fradkin, J.; et al. Update on Prevention of Cardiovascular Disease in Adults with Type 2 Diabetes Mellitus in Light of Recent Evidence: A Scientific Statement from the American Heart Association and the American Diabetes Association. Circulation 2015, 132, 691–718. [Google Scholar] [CrossRef]
- Low Wang, C.C.; Hess, C.N.; Hiatt, W.R.; Goldfine, A.B. Clinical Update: Cardiovascular Disease in Diabetes Mellitus. Circulation 2016, 133, 2459–2502. [Google Scholar] [CrossRef]
- Milicevic, Z.; Raz, I.; Beattie, S.D.; Campaigne, B.N.; Sarwat, S.; Gromniak, E.; Kowalska, I.; Galic, E.; Tan, M.; Hanefeld, M. Natural History of Cardiovascular Disease in Patients with Diabetes: Role of Hyperglycemia. Diabetes Care 2008, 31 (Suppl. S2), S155–S160. [Google Scholar] [CrossRef]
- Rosengren, A.; Dikaiou, P. Cardiovascular Outcomes in Type 1 and Type 2 Diabetes. Diabetologia 2023, 66, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.; Bostrom, J.A.; Buysschaert, M.; Newman, J.D.; Goldberg, I.J.; Bergman, M. Diabetes Research and Clinical Practice Management of Dyslipidemia and Atherosclerotic Cardiovascular Risk in Prediabetes. Diabetes Res. Clin. Pract. 2022, 190, 109980. [Google Scholar] [CrossRef]
- Ertürk Zararsız, G.; Bolat, S.; Cephe, A.; Kochan, N.; Yerlitaş, S.İ.; Doğan, H.O.; Zararsız, G. Validation of Friedewald, Martin-Hopkins and Sampson Low-Density Lipoprotein Cholesterol Equations. PLoS ONE 2022, 17, e0263860. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, H.N.; Rosenson, R.S.; Kees Hovingh, G.; Letierce, A.; Samuel, R.; Poulouin, Y.; Cannon, C.P. LDL-C Calculated by Friedewald, Martin-Hopkins, or NIH Equation 2 versus Beta-Quantification: Pooled Alirocumab Trials. J. Lipid Res. 2022, 63, 100148. [Google Scholar] [CrossRef]
- Sampson, M.; Ling, C.; Sun, Q.; Harb, R.; Ashmaig, M.; Warnick, R.; Sethi, A.; Fleming, J.K.; Otvos, J.D.; Meeusen, J.W.; et al. A New Equation for Calculation of Low-Density Lipoprotein Cholesterol in Patients with Normolipidemia and/or Hypertriglyceridemia. JAMA Cardiol. 2020, 5, 540–548. [Google Scholar] [CrossRef]
- Van Deventer, H.E.; Miller, W.G.; Myers, G.L.; Sakurabayashi, I.; Bachmann, L.M.; Caudill, S.P.; Dziekonski, A.; Edwards, S.; Kimberly, M.M.; Korzun, W.J.; et al. Non-HDL Cholesterol Shows Improved Accuracy for Cardiovascular Risk Score Classification Compared to Direct or Calculated LDL Cholesterol in a Dyslipidemic Population. Clin. Chem. 2011, 57, 490–501. [Google Scholar] [CrossRef]
- Filippatos, T.; Tsimihodimos, V.; Pappa, E.; Elisaf, M. Pathophysiology of Diabetic Dyslipidaemia. Curr. Vasc. Pharmacol. 2017, 15, 566–575. [Google Scholar] [CrossRef]
- Glavinovic, T.; Thanassoulis, G.; de Graaf, J.; Couture, P.; Hegele, R.A.; Sniderman, A.D. Physiological Bases for the Superiority of Apolipoprotein B Over Low-Density Lipoprotein Cholesterol and Non–HighDensity Lipoprotein Cholesterol as a Marker of Cardiovascular Risk. J. Am. Heart Assoc. 2022, 11, e025858. [Google Scholar] [CrossRef]
- Srisurin, W. The Reliability of Calculated Low-Density Lipoprotein Cholesterol from Four Different Formulas in Thai Diabetic Patients. J. Med. Assoc. Thail. 2014, 97, 97. [Google Scholar]
- Chaen, H.; Kinchiku, S.; Miyata, M.; Kajiya, S.; Uenomachi, H.; Yuasa, T.; Takasaki, K.; Ohishi, M. Validity of a Novel Method for Estimation of Low-Density Lipoprotein Cholesterol Levels in Diabetic Patients. J. Atheroscler. Thromb. 2016, 23, 1355–1364. [Google Scholar] [CrossRef]
- Kurniawan, L.B.; Windarwati, W.; Mulyono, B. Analysis of Ldl-C Measurement Using Direct and Friedewald Formula in Type 2 Diabetes Mellitus Patients. Indones. J. Clin. Pathol. Med. Lab. 2018, 24, 255. [Google Scholar] [CrossRef]
- Razi, F.; Forouzanfar, K.; Bandarian, F.; Nasli-Esfahani, E. LDL-Cholesterol Measurement in Diabetic Type 2 Patients: A Comparison between Direct Assay and Popular Equations. J. Diabetes Metab. Disord. 2017, 16, 43. [Google Scholar] [CrossRef] [PubMed]
- Sibal, L.; Neely, R.D.G.; Jones, A.; Home, P.D. Friedewald Equation Underestimates Low-Density Lipoprotein Cholesterol at Low Concentrations in Young People with and without Type 1 Diabetes. Diabet. Med. 2010, 27, 37–45. [Google Scholar] [CrossRef]
- Naser, A.; Isgandarov, K.; Güvenç, T.S.; Güvenç, R.Ç. Original Article Comparison of Novel Martin/Hopkins and Sampson Equations for Calculation of Low-Density Lipoprotein Cholesterol in Diabetic Patients. Arq. Bras. Cardiol. 2022, 119, 225–233. [Google Scholar]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Martin, S.S.; Blaha, M.J.; Elshazly, M.B.; Toth, P.P.; Kwiterovich, P.O.; Blumenthal, R.S.; Jones, S.R. Comparison of a Novel Method vs the Friedewald Equation for Estimating Low-Density Lipoprotein Cholesterol Levels from the Standard Lipid Profile. JAMA J. Am. Med. Assoc. 2013, 310, 2061–2068. [Google Scholar] [CrossRef]
- Sajja, A.; Park, J.; Sathiyakumar, V.; Varghese, B.; Pallazola, V.A.; Marvel, F.A.; Kulkarni, K.; Muthukumar, A.; Joshi, P.H.; Gianos, E.; et al. Comparison of Methods to Estimate Low-Density Lipoprotein Cholesterol in Patients with High Triglyceride Levels. JAMA Netw. Open 2021, 4, e2128817. [Google Scholar] [CrossRef]
- Esawy, M.M.; Shabana, M.A.; Magdy, M.M. Evaluation of Martin’s Equation for LDL-C Estimation in Type 2 Diabetes Mellitus Egyptian Patients. Clin. Chim. Acta 2019, 495, 487–492. [Google Scholar] [CrossRef]
- Tomo, S.; Sankanagoudar, S.; Shukla, R.; Sharma, P. Validation of a Novel Method for Determination of Low-Density Lipoprotein Cholesterol Levels in Indian Patients with Type 2 Diabetes. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102448. [Google Scholar] [CrossRef]
- Masson, W.; Huerín, M.; Lobo, M.; Masson, G.; Webmaster, D.; Fernández, N.; Micali, G.; Nemec, M.; Romero, C.; Molinero, G.; et al. Lipid Goals in Diabetic Patients. Clinical Implications after Application of a New Formula for Ldl-Cholesterol Calculation. Rev. Argent. Cardiol. 2020, 88, 39–45. [Google Scholar] [CrossRef]
- Choi, S.Y.; Park, H.E.; Kim, M.K.; Shin, C.S.; Cho, S.H.; Oh, B.H. Difference between Calculated and Direct-Measured Low-Density Lipoprotein Cholesterol in Subjects with Diabetes Mellitus or Taking Lipid-Lowering Medications. J. Clin. Lipidol. 2012, 6, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Hirany, S.; Li, D.; Jialal, I. A More Valid Measurement of Low-Density Lipoprotein Cholesterol in Diabetic Patients. Am. J. Med. 1997, 102, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Wägner, A.M.; Sánchez_quesada, J.L.; Pérez, A.; Rigla, M.; Cortés, M.; Blanco-Vaca, F.; Ordóñez-Llanos, J. Diabetes: Consequences for Patient Risk Classification. Clin. Chem. 2000, 46, 1830–1832. [Google Scholar] [CrossRef] [PubMed]
- Rubiés-Prat, J.; Reverter, J.L.; Sentí, M.; Pedro-Botet, J.; Salinas, I.; Lucas, A.; Nogués, X.; Sanmartí, A. Calculated low-density lipoprotein cholesterol should not be used for management of lipoprotein abnormalities in patients with diabetes mellitus. Diabetes Care 1993, 16, 1081–1086. [Google Scholar] [CrossRef]
- Whiting, L.J.; Shephard, M.D.S.; Tallis, G.A. Measurement of Plasma LDL Cholesterol in Patients with Diabetes. Diabetes Care 1997, 20, 12–14. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 6. Glycemic Targets: Standards of Medical Care in Diabetesd—2019. Diabetes Care 2019, 42, S61–S70. [Google Scholar] [CrossRef]
- Gagel, A.; Zghyer, F.; Samuel, C.; Martin, S.S. What Is the Optimal Low-Density Lipoprotein Cholesterol? Med. Clin. N. Am. 2022, 106, 285–298. [Google Scholar] [CrossRef]
- Watts, G.F.; Barrett, P.H.R.; Ji, J.; Serone, A.P.; Chan, D.C.; Croft, K.D.; Loehrer, F.; Johnson, A.G. Differential Regulation of Lipoprotein Kinetics by Atorvastatin and Fenofibrate in Subjects with the Metabolic Syndrome. Diabetes 2003, 52, 803–811. [Google Scholar] [CrossRef]
- Chan, D.C.; Watts, G.F.; Redgrave, T.G.; Mori, T.A.; Barrett, P.H.R. Apolipoprotein B-100 Kinetics in Visceral Obesity: Associations with Plasma Apolipoprotein C-III Concentration. Metabolism 2002, 51, 1041–1046. [Google Scholar] [CrossRef]
- Riches, F.M.; Watts, G.F.; Naoumova, R.P.; Kelly, J.M.; Croft, K.D.; Thompson, G.R. Hepatic Secretion of Very-Low-Density Lipoprotein Apolipoprotein B-100 Studied with a Stable Isotope Technique in Men with Visceral Obesity. Int. J. Obes. 1998, 22, 414–423. [Google Scholar] [CrossRef]
- Ćwiklińska, A.; Wieczorek, E.; Gliwińska, A.; Marcinkowska, M.; Czaplińska, M.; Mickiewicz, A.; Kuchta, A.; Kortas-Stempak, B.; Gruchała, M.; Dȩbska-Ślizień, A.; et al. Non-HDL-C/TG Ratio Indicates Significant Underestimation of Calculated Low-Density Lipoprotein Cholesterol (LDL-C) Better than TG Level: A Study on the Reliability of Mathematical Formulas Used for LDL-C Estimation. Clin. Chem. Lab. Med. 2021, 59, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Fogacci, F.; Patrono, D.; Mancini, R.; Ramazzotti, E.; Borghi, C.; D’Addato, S.; Bove, M.; Piani, F.; Giovannini, M.; et al. Application of the Sampson Equation to Estimate LDL-C in Children: Comparison with LDL Direct Measurement and Friedewald Equation in the BLIP Study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, P1911–P1915. [Google Scholar] [CrossRef] [PubMed]
- Piani, F.; Cicero, A.F.G.; Ventura, F.; Dormi, A.; Fogacci, F.; Patrono, D.; Mancini, R.; Ramazzotti, E.; Borghi, C.; D’Addato, S.; et al. Evaluation of Twelve Formulas for LDL-C Estimation in a Large, Blinded, Random Italian Population. Int. J. Cardiol. 2021, 330, 221–227. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TG Levels (mg/dL) | Non-HDL-C (mg/dL) | |||||
|---|---|---|---|---|---|---|
| <100 | 100–129 | 130–159 | 160–189 | 190–219 | ≥220 | |
| 7–49 | 8.17 | 6.62 | 5.00 | 4.36 | - | 14.67 |
| 50–56 | 9.00 | 7.00 | 5.58 | 3.50 | - | 3.53 |
| 57–61 | 8.50 | 8.14 | 6.33 | 5.45 | 6.56 | - |
| 62–66 | 8.13 | 7.33 | 7.33 | 5.13 | 4.14 | - |
| 67–71 | 9.57 | 7.67 | 6.18 | 5.65 | 4.38 | 17.00 |
| 72–75 | 9.25 | 8.00 | 7.40 | 7.40 | 7.90 | 18.25 |
| 76–69 | 9.50 | 7.80 | 5.57 | 7.18 | 12.61 | 8.53 |
| 80–83 | 9.22 | 8.20 | 7.55 | 8.15 | 4.78 | 4.21 |
| 84–87 | 8.70 | 8.70 | 7.08 | 5.73 | 4.63 | 8.07 |
| 88–92 | 8.80 | 8.80 | 7.08 | 5.75 | 5.80 | 10.49 |
| 93–96 | 8.73 | 8.64 | 8.00 | 6.00 | 5.00 | 5.00 |
| 97–100 | 9.00 | 8.82 | 8.25 | 6.39 | 5.50 | 28.58 |
| 101–105 | 8.58 | 8.58 | 8.67 | 6.80 | 6.59 | 20.20 |
| 106–110 | 9.00 | 8.38 | 8.46 | 8.04 | 5.43 | 4.98 |
| 111–115 | 8.85 | 8.77 | 8.62 | 7.60 | 6.53 | 5.81 |
| 116–120 | 9.45 | 8.54 | 8.54 | 7.44 | 6.16 | 5.02 |
| 121–126 | 9.38 | 9.00 | 8.23 | 7.41 | 7.24 | 6.78 |
| 127–132 | 8.60 | 9.21 | 8.19 | 7.17 | 6.07 | 5.74 |
| 133–138 | 8.50 | 9.20 | 8.53 | 8.38 | 6.14 | 5.52 |
| 139–146 | 8.75 | 9.00 | 8.59 | 8.24 | 6.64 | 6.67 |
| 147–154 | 9.34 | 9.06 | 8.65 | 8.05 | 6.61 | 8.82 |
| 155–163 | 9.38 | 9.35 | 8.72 | 8.00 | 7.62 | 7.11 |
| 164–173 | 9.56 | 9.36 | 8.45 | 7.59 | 7.64 | 6.59 |
| 174–185 | 8.70 | 9.50 | 8.71 | 7.96 | 6.96 | 6.81 |
| 186–201 | 9.75 | 9.07 | 8.88 | 8.28 | 7.14 | 7.11 |
| 202–220 | 8.87 | 9.32 | 8.90 | 8.23 | 7.77 | 6.79 |
| 221–247 | 8.54 | 9.40 | 8.77 | 8.54 | 8.18 | 7.59 |
| 248–292 | 8.93 | 9.18 | 8.69 | 8.39 | 7.61 | 7.30 |
| 293–399 | 8.59 | 9.11 | 8.68 | 8.11 | 7.65 | 7.15 |
| ≥400 | 9.80 | 9.08 | 8.69 | 7.99 | 7.32 | 6.57 |
| Characteristic | Group | Diabetic Group | |||||
|---|---|---|---|---|---|---|---|
| Non-Diabetic (N = 11,423) | Prediabetic (N = 9362) | Diabetic (N = 10,246) | p | Uncontrolled (N = 7452) | Controlled (N = 2794) | p | |
| Age (years) | 43.57 ± 16.48 a | 56.97 ± 14.19 b | 61.12 ± 12.43 c | <0.001 | 60.78 ± 12.45 | 61.99 ± 12.34 | <0.001 |
| Sex | |||||||
| Female | 7276 (63.7) a | 5583 (59.6) b | 5768 (56.3) c | <0.001 | 4174 (56.0) | 1594 (57.1) | 0.892 |
| Male | 4147 (36.3) a | 3779 (40.4) b | 4478 (43.7) c | 3278 (44.0) | 1200 (42.9) | ||
| Lipid values | |||||||
| TC (mg/dL) | 176.00 (152.00–204.00) a | 186.00 (157.00–215.00) b | 178.00 (149.00–210.00) c | <0.001 | 178.00 (149.00–210.00) | 178.00 (148.00–208.00) | 0.164 |
| TG (mg/dL) | 116.00 (83.00–165.00) a | 139.00 (100.00–193.00) b | 155.00 (111.00–221.00) c | <0.001 | 159.00 (113.00–229.00) | 146.00 (107.00–201.25) | <0.001 |
| HDL-C (mg/dL) | 46.00 (39.00–56.00) a | 44.00 (37.00–52.00) b | 41.00 (34.75–49.00) c | <0.001 | 41.00 (34.00–49.00) | 42.00 (36.00–50.00) | <0.001 |
| Non-HDL-C (mg/dL) | 127.00 (103.00–155.00) a | 140.00 (113.00–169.00) b | 134.00 (107.00–166.00) c | <0.001 | 135.00 (107.00–167.00) | 134.00 (104.00–162.25) | 0.002 |
| TG-TC ratio | 0.66 (0.50–0.93) a | 0.76 (0.58–1.02) b | 0.89 (0.67–1.22) c | <0.001 | 0.92 (0.68–1.25) | 0.85 (0.64–1.12) | <0.001 |
| LDL-C(D) (mg/dL) | 112.00 (90.00–136.00) a | 121.00 (96.00–146.00) b | 113.00 (87.00–139.00) a | <0.001 | 113.00 (88.00–140.00) | 113.00 (86.00–138.00) | 0.467 |
| LDL-C(F) (mg/dL) | 101.00 (79.80–124.40) a | 108.60 (84.60–132.60) b | 99.00 (75.00–124.80) c | <0.001 | 98.60 (74.80–124.60) | 100.20 (75.40–125.25) | 0.306 |
| LDL-C(S) (mg/dL) | 103.79 (82.60–127.19) a | 112.24 (88.37–135.85) b | 103.41 (79.62–128.60) a | <0.001 | 103.07 (79.72–128.49) | 104.20 (79.29–129.06) | 0.717 |
| LDL-C(M) (mg/dL) | 104.13 (82.92–127.55) a | 113.30 (90.07–137.13) b | 105.98 (82.08–131.14) c | <0.001 | 105.85 (82.67–131.37) | 106.23 (80.70–130.52) | 0.385 |
| LDL-C(E) (mg/dL) | 112.00 (90.33–135.68) a | 121.17 (97.62–145.78) b | 113.95 (89.36–139.42) c | <0.001 | 113.58 (89.44–139.25) | 114.01 (87.93–138.58) | 0.612 |
| Non-HDL-C-TG ratio | 2.46 (1.82–3.23) a | 2.24 (1.70–2.92) b | 1.91 (1.43–2.52) c | <0.001 | - | - | - |
| Remnant-C(D) (mg/dL) | 14.00 (8.00–22.00) a | 17.00 (10.00–26.00) b | 19.00 (11.00–29.00) c | <0.001 | - | - | - |
| LDL-C | LDL-C Estimating Equations | |||
|---|---|---|---|---|
| Friedewald | Sampson | Martin–Hopkins | Extended Martin–Hopkins | |
| LDL-C | ||||
| <70 mg/dL | 78.7 | 84.7 | 83.5 | 77.8 |
| ≥70 mg/dL | 89.9 | 93.5 | 95.7 | 98.7 |
| LDL-C | ||||
| <100 mg/dL | 92.5 | 94.4 | 93.6 | 88.3 |
| ≥100 mg/dL | 76.0 | 83.0 | 86.5 | 95.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolat, S.; Ertürk Zararsız, G.; Doğan, K.; Kochan, N.; Yerlitaş, S.I.; Cephe, A.; Zararsız, G.; Cicero, A.F.G. Concordance of LDL-C Estimating Equations with Direct Enzymatic Measurement in Diabetic and Prediabetic Subjects. J. Clin. Med. 2023, 12, 3570. https://doi.org/10.3390/jcm12103570
Bolat S, Ertürk Zararsız G, Doğan K, Kochan N, Yerlitaş SI, Cephe A, Zararsız G, Cicero AFG. Concordance of LDL-C Estimating Equations with Direct Enzymatic Measurement in Diabetic and Prediabetic Subjects. Journal of Clinical Medicine. 2023; 12(10):3570. https://doi.org/10.3390/jcm12103570
Chicago/Turabian StyleBolat, Serkan, Gözde Ertürk Zararsız, Kübra Doğan, Necla Kochan, Serra I. Yerlitaş, Ahu Cephe, Gökmen Zararsız, and Arrigo F. G. Cicero. 2023. "Concordance of LDL-C Estimating Equations with Direct Enzymatic Measurement in Diabetic and Prediabetic Subjects" Journal of Clinical Medicine 12, no. 10: 3570. https://doi.org/10.3390/jcm12103570