
Syphilis as Re-Emerging Disease, Antibiotic Resistance, and Vulnerable Population: Global Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Extraction
2.2. Statistical Analysis
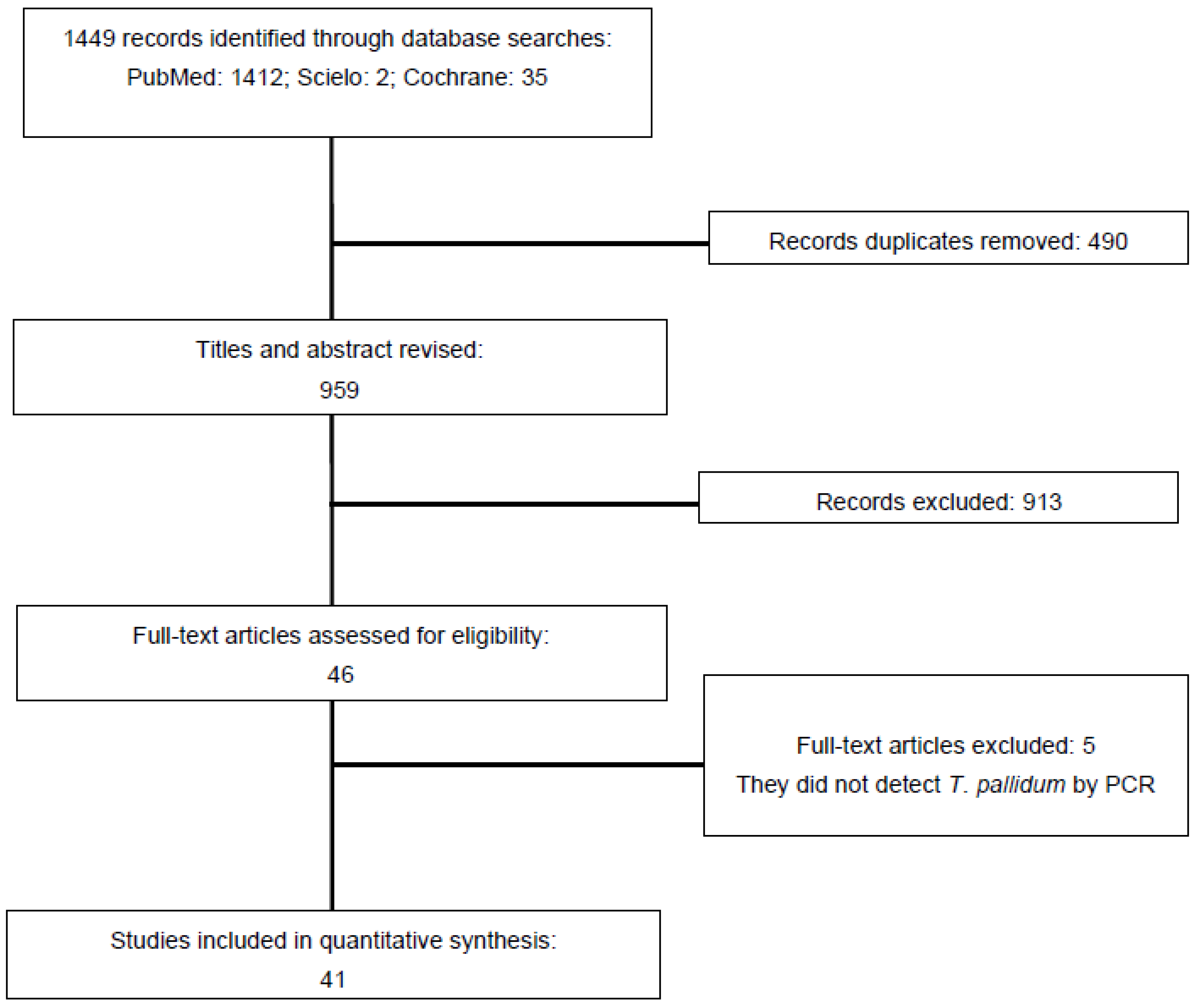
3. Results
3.1. Characteristics of Study Eligible
3.2. Bias Risk Assessment
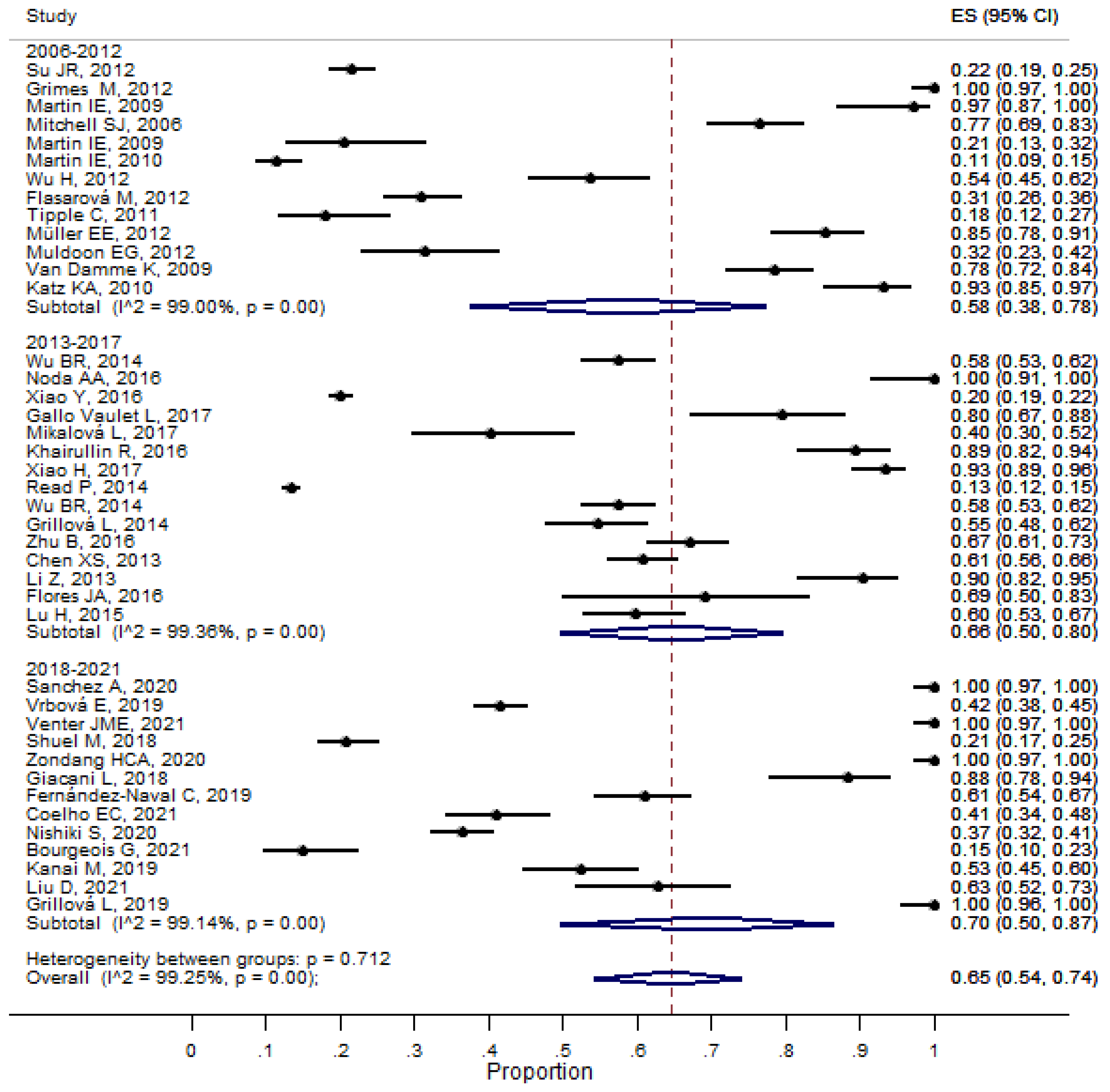
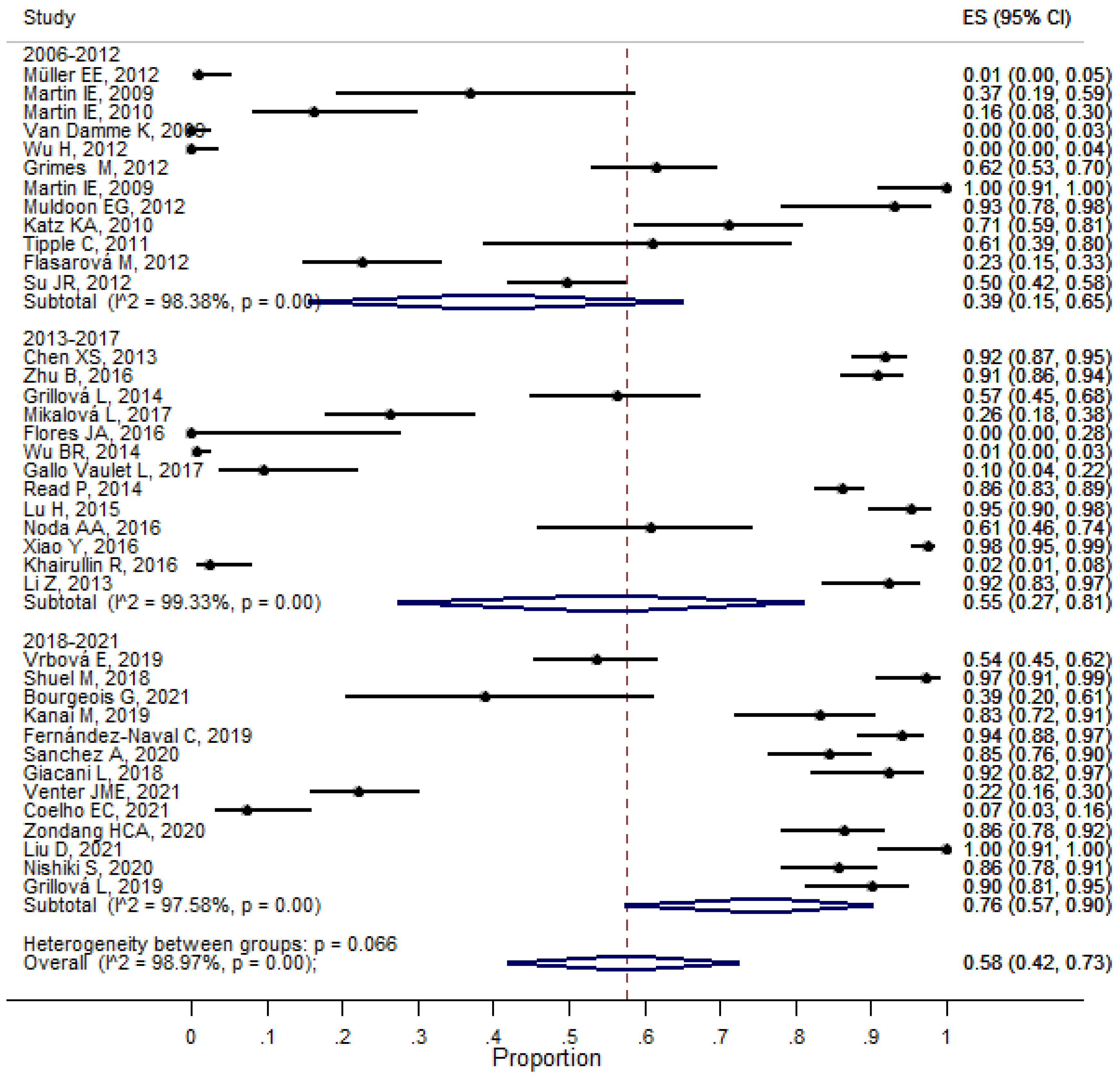
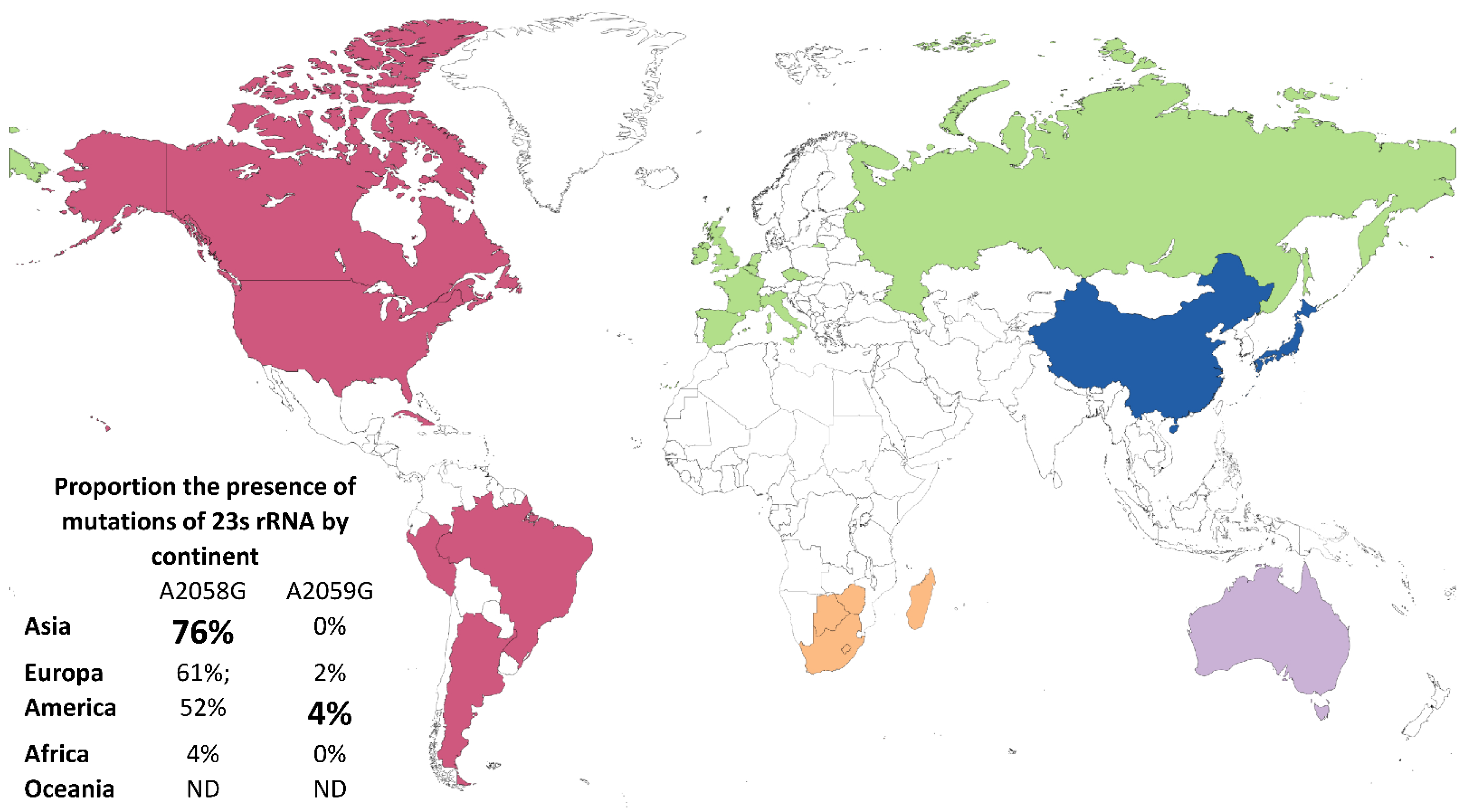
3.3. Meta-Analysis of Proportion of Syphilis and Antibiotic Resistance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nokhodian, Z.; Yazdani, M.R.; Yaran, M.; Shoaei, P.; Mirian, M.; Ataei, B.; Babak, A.; Ataie, M. Prevalence and Risk Factors of HIV, Syphilis, Hepatitis B and C among Female Prisoners in Isfahan, Iran. Hepat. Mon. 2012, 12, 442–447. [Google Scholar] [CrossRef] [Green Version]
- Clark, J.L.; Caceres, C.F.; Lescano, A.G.; Konda, K.A.; Leon, S.R.; Jones, F.R.; Kegeles, S.M.; Klausner, J.D.; Coates, T.J. NIMH STD/HIV Collaborative Prevention Trial Prevalence of Same-Sex Sexual Behavior and Associated Characteristics among Low-Income Urban Males in Peru. PLoS ONE 2007, 2, e778. [Google Scholar] [CrossRef] [Green Version]
- Chan, P.A.; Hogan, J.W.; Huang, A.; DeLong, A.; Salemi, M.; Mayer, K.H.; Kantor, R. Phylogenetic Investigation of a Statewide HIV-1 Epidemic Reveals Ongoing and Active Transmission Networks among Men Who Have Sex with Men. J. Acquir. Immune Defic. Syndr. 1999 2015, 70, 428–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoni, A.C.; González, M.A.; Sjögren, H.W. Syphilis in the most at-risk populations in Latin America and the Caribbean: A systematic review. Int. J. Infect. Dis. 2013, 17, e84–e92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syphilis—Level 4 Cause. Available online: https://www.healthdata.org/results/gbd_summaries/2019/syphilis-level-4-cause (accessed on 1 November 2022).
- New Study Highlights Unacceptably High Global Prevalence of Syphilis among Men Who Have Sex with Men. Available online: https://www.who.int/news/item/09-07-2021-new-study-highlights-unacceptably-high-global-prevalence-of-syphilis-among-men-who-have-sex-with-men (accessed on 1 November 2022).
- Medina, M.M.; Crowley, C.; Montgomery, M.C.; Tributino, A.; Almonte, A.; Sowemimo-Coker, G.; Nunn, A.; Chan, P.A. Disclosure of HIV Serostatus and Pre-exposure Prophylaxis Use on Internet Hookup Sites among Men Who Have Sex with Men. AIDS Behav. 2019, 23, 1681–1688. [Google Scholar] [CrossRef] [PubMed]
- Syphilis—Annual Epidemiological Report for 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/syphilis-annual-epidemiological-report-2018 (accessed on 1 November 2022).
- Viciana, I.; González-Domenech, C.M.; Palacios, R.; Delgado, M.; Del Arco, A.; Tellez, F.; Jarilla, F.; Fernández, S.; Clavijo, E.; Santos, J. Clinical, virological and phylogenetic characterization of a multiresistant HIV-1 strain outbreak in naive patients in southern Spain. J. Antimicrob. Chemother. 2016, 71, 357–361. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Xie, Y.; Xiao, Y. Laboratory Diagnostic Tools for Syphilis: Current Status and Future Prospects. Front. Cell Infect. Microbiol. 2021, 10, 574806. [Google Scholar] [CrossRef]
- Zhou, P.; Li, K.; Lu, H.; Qian, Y.; Gu, X.; Gong, W.; Tucker, J.D.; Cohen, M.S. Azithromycin treatment failure among primary and secondary syphilis patients in Shanghai. Sex. Transm. Dis. 2010, 37, 726–729. [Google Scholar] [CrossRef] [Green Version]
- Noda, A.A.; Matos, N.; Blanco, O.; Rodríguez, I.; Stamm, L.V. First Report of the 23S rRNA Gene A2058G Point Mutation Associated with Macrolide Resistance in Treponema pallidum from Syphilis Patients in Cuba. Sex. Transm. Dis. 2016, 43, 332–334. [Google Scholar] [CrossRef]
- Shukalek, C.B.; Lee, B.; Fathima, S.; Chu, A.; Fonseca, K.; Somayaji, R. Comparative Analysis of Molecular and Serologic Testing for Primary Syphilis: A Population-Based Cohort Study. Front. Cell Infect. Microbiol. 2021, 11, 579660. [Google Scholar] [CrossRef]
- Workowski, K.A.; Bachmann, L.H.; Chan, P.A.; Johnston, C.M.; Muzny, C.A.; Park, I.; Reno, H.; Zenilman, J.M.; Bolan, G.A. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm. Rep. 2021, 70, 1–187. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Regional Office for the Western Pacific. Review of National Treatment Guidelines for Sexually Transmitted Infections in the Western Pacific Region [Fact Sheet]; Report No.: WPR/2018/DCD/004; WHO Regional Office for the Western Pacific: Manila, Philippines, 2018; Available online: https://apps.who.int/iris/handle/10665/279732 (accessed on 1 November 2022).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Ottawa Hospital Research Institute. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 November 2022).
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.W. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions. 2°; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- World Bank Country and Lending Groups—World Bank Data Help Desk. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 1 November 2022).
- Harbord, R.M.; Egger, M.; Sterne, J.A.C. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat. Med. 2006, 25, 3443–3457. [Google Scholar] [CrossRef]
- Coelho, E.C.; Souza, S.B.; Costa, C.C.S.; Costa, L.M.; Pinheiro, L.M.L.; Machado, L.F.A.; Silva-Oliveira, G.C.; Martins, L.C.; Frade, P.C.R.; Oliveira-Filho, A.B. Treponema pallidum in female sex workers from the Brazilian Marajó Archipelago: Prevalence, risk factors, drug-resistant mutations and coinfections. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 792–800. [Google Scholar] [CrossRef]
- Mikalová, L.; Grillová, L.; Osbak, K.; Strouhal, M.; Kenyon, C.; Crucitti, T.; Šmajs, D. Molecular Typing of Syphilis-Causing Strains among Human Immunodeficiency Virus-Positive Patients in Antwerp, Belgium. Sex. Transm. Dis. 2017, 44, 376–379. [Google Scholar] [CrossRef]
- Liu, D.; He, S.M.; Zhu, X.Z.; Liu, L.L.; Lin, L.R.; Niu, J.J.; Yang, T.C. Molecular Characterization Based on MLST and ECDC Typing Schemes and Antibiotic Resistance Analyses of Treponema pallidum subsp. pallidum in Xiamen, China. Front. Cell. Infect. Microbiol. 2021, 10, 618747. [Google Scholar] [CrossRef]
- Bourgeois, G.; Grange, P.; Saint-Pastou Terrier, C.; Koumar, Y.; Manaquin, R.; Zemali, N.; Poubeau, P.; Dupin, N.; Jaubert, J.; Bertolotti, A. Azithromycin resistance in Treponema pallidum in Reunion Island: A cross-sectional study. Ann. Dermatol. Venereol. 2021, 148, 165–167. [Google Scholar] [CrossRef]
- Mitchell, S.J.; Engelman, J.; Kent, C.K.; Lukehart, S.A.; Godornes, C.; Klausner, J.D. Azithromycin-Resistant Syphilis Infection: San Francisco, California, 2000–2004. Clin. Infect. Dis. 2006, 42, 337–345. [Google Scholar] [CrossRef]
- Read, P.; Jeoffreys, N.; Tagg, K.; Guy, R.J.; Gilbert, G.L.; Donovan, B. Azithromycin-resistant syphilis-causing strains in Sydney, Australia: Prevalence and risk factors. J. Clin. Microbiol. 2014, 52, 2776–2781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Naval, C.; Arando, M.; Espasa, M.; Antón, A.; Fernández-Huerta, M.; Silgado, A.; Jimenez, I.; Villatoro, A.M.; González-López, J.J.; Serra-Pladevall, J.; et al. Enhanced molecular typing and macrolide and tetracycline-resistance mutations of Treponema pallidum in Barcelona. Future Microbiol. 2019, 14, 1099–1108. [Google Scholar] [CrossRef] [PubMed]
- Giacani, L.; Ciccarese, G.; Puga-Salazar, C.; Dal Conte, I.; Colli, L.; Cusini, M.; Ramoni, S.; Delmonte, S.; D’Antuono, A.; Gaspari, V.; et al. Enhanced Molecular Typing of Treponema pallidum subspecies pallidum Strains from 4 Italian Hospitals Shows Geographical Differences in Strain Type Heterogeneity, Widespread Resistance to Macrolides, and Lack of Mutations Associated with Doxycycline Resistance. Sex. Transm. Dis. 2018, 45, 237–242. [Google Scholar] [PubMed]
- Nishiki, S.; Arima, Y.; Kanai, M.; Shimuta, K.; Nakayama, S.-I.; Ohnishi, M. Epidemiology, molecular strain types, and macrolide resistance of Treponema pallidum in Japan, 2017–2018. J. Infect. Chemother. Off. J. Jpn. Soc. Chemother. 2020, 26, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Van Damme, K.; Behets, F.; Ravelomanana, N.; Godornes, C.; Khan, M.; Randrianasolo, B.; Rabenja, N.L.; Lukehart, S.; Cohen, M.; Hook, E. Evaluation of azithromycin resistance in Treponema pallidum specimens from Madagascar. Sex. Transm. Dis. 2009, 36, 775–776. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Chang, S.-Y.; Lee, N.-Y.; Huang, W.-C.; Wu, B.-R.; Yang, C.-J.; Liang, S.-H.; Lee, C.-H.; Ko, W.-C.; Lin, H.-H.; et al. Evaluation of macrolide resistance and enhanced molecular typing of Treponema pallidum in patients with syphilis in Taiwan: A prospective multicenter study. J. Clin. Microbiol. 2012, 50, 2299–2304. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.; Li, K.; Gong, W.; Yan, L.; Gu, X.; Chai, Z.; Guan, Z.; Zhou, P. High frequency of the 23S rRNA A2058G mutation of Treponema pallidum in Shanghai is associated with a current strategy for the treatment of syphilis. Emerg. Microbes Infect. 2015, 4, e10. [Google Scholar] [CrossRef]
- Chen, X.-S.; Yin, Y.-P.; Wei, W.-H.; Wang, H.-C.; Peng, R.-R.; Zheng, H.-P.; Zhang, J.-P.; Zhu, B.-Y.; Liu, Q.-Z.; Huang, S.-J. High prevalence of azithromycin resistance to Treponema pallidum in geographically different areas in China. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2013, 19, 975–979. [Google Scholar] [CrossRef] [Green Version]
- Tipple, C.; McClure, M.O.; Taylor, G.P. High prevalence of macrolide resistant Treponema pallidum strains in a London centre. Sex. Transm. Infect. 2011, 87, 486–488. [Google Scholar] [CrossRef]
- Zhu, B.; Bu, J.; Li, W.; Zhang, J.; Huang, G.; Cao, J.; Tang, Z.; Gan, Q.; Wei, P. High Resistance to Azithromycin in Clinical Samples from Patients with Sexually Transmitted Diseases in Guangxi Zhuang Autonomous Region, China. PLoS ONE 2016, 11, e0159787. [Google Scholar] [CrossRef] [Green Version]
- Martin, I.E.; Gu, W.; Yang, Y.; Tsang, R.S.W. Macrolide Resistance and Molecular Types of Treponema pallidum Causing Primary Syphilis in Shanghai, China. Clin. Infect. Dis. 2009, 49, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, E.E.; Paz-Bailey, G.; Lewis, D.A. Macrolide resistance testing and molecular subtyping of Treponema pallidum strains from Southern Africa. Sex. Transm. Infect. 2012, 88, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Vrbová, E.; Grillová, L.; Mikalová, L.; Pospíšilová, P.; Strnadel, R.; Dastychová, E.; Kojanová, M.; Kreidlová, M.; Vaňousová, D.; Rob, F.; et al. MLST typing of Treponema pallidum subsp. pallidum in the Czech Republic during 2004–2017: Clinical isolates belonged to 25 allelic profiles and harbored 8 novel allelic variants. PLoS ONE 2019, 14, e0217611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zondag, H.C.A.; Cornelissen, A.R.; van Dam, A.P.; Bruisten, S.M. Molecular diversity of Treponema pallidum subspecies pallidum isolates in Amsterdam, the Netherlands. Sex. Transm. Infect. 2020, 96, 223–226. [Google Scholar] [CrossRef] [Green Version]
- Katz, K.A.; Pillay, A.; Ahrens, K.; Kohn, R.P.; Hermanstyne, K.; Bernstein, K.T.; Ballard, R.C.; Klausner, J.D. Molecular epidemiology of syphilis—San Francisco, 2004–2007. Sex. Transm. Dis. 2010, 37, 660–663. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Y.; Liu, S.; Liu, Z.; Xie, Y.; Jiang, C.; Xu, M.; Zhao, F.; Zeng, T.; Yu, J.; Wu, Y. Molecular Subtyping and Surveillance of Resistance Genes in Treponema pallidum DNA from Patients with Secondary and Latent Syphilis in Hunan, China. Sex. Transm. Dis. 2016, 43, 310–316. [Google Scholar] [CrossRef]
- Kanai, M.; Arima, Y.; Nishiki, S.; Shimuta, K.; Itoda, I.; Matsui, T.; Oishi, K.; Ohnishi, M.; Nakayama, S.-I. Molecular Typing and Macrolide Resistance Analyses of Treponema pallidum in Heterosexuals and Men Who Have Sex with Men in Japan, 2017. J. Clin. Microbiol. 2019, 57, e01167-18. [Google Scholar] [CrossRef] [Green Version]
- Shuel, M.; Hayden, K.; Kadkhoda, K.; Tsang, R.S.W. Molecular Typing and Macrolide Resistance of Syphilis Cases in Manitoba, Canada, from 2012 to 2016. Sex. Transm. Dis. 2018, 45, 233–236. [Google Scholar] [CrossRef] [Green Version]
- Grillová, L.; Pĕtrošová, H.; Mikalová, L.; Strnadel, R.; Dastychová, E.; Kuklová, I.; Kojanová, M.; Kreidlová, M.; Vaňousová, D.; Hercogová, J.; et al. Molecular typing of Treponema pallidum in the Czech Republic during 2011 to 2013: Increased prevalence of identified genotypes and of isolates with macrolide resistance. J. Clin. Microbiol. 2014, 52, 3693–3700. [Google Scholar] [CrossRef] [Green Version]
- Gallo Vaulet, L.; Grillová, L.; Mikalová, L.; Casco, R.; Rodríguez Fermepin, M.; Pando, M.A.; Šmajs, D. Molecular typing of Treponema pallidum isolates from Buenos Aires, Argentina: Frequent Nichols-like isolates and low levels of macrolide resistance. PLoS ONE 2017, 12, e0172905. [Google Scholar] [CrossRef]
- Martin, I.E.; Tsang, R.S.W.; Sutherland, K.; Anderson, B.; Read, R.; Roy, C.; Yanow, S.; Fonseca, K.; White, W.; Kandola, K.; et al. Molecular typing of Treponema pallidum strains in western Canada: Predominance of 14d subtypes. Sex. Transm. Dis. 2010, 37, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.-R.; Liu, W.-C.; Wu, P.-Y.; Su, Y.-C.; Yang, S.-P.; Hung, C.-C.; Chang, S.-Y. Surveillance study of Treponema pallidum harbouring tetracycline resistance mutations in patients with syphilis. Int. J. Antimicrob. Agents 2014, 44, 370–372. [Google Scholar] [CrossRef] [PubMed]
- Grillová, L.; Noda, A.A.; Lienhard, R.; Blanco, O.; Rodríguez, I.; Šmajs, D. Multilocus Sequence Typing of Treponema pallidum subsp. pallidum in Cuba from 2012 to 2017. J. Infect. Dis. 2019, 219, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Li, Z.; Li, F.; Wen, J.; Liu, D.; Du, W.; Hou, J.; Li, Z.; Zheng, R.; Liu, D.; et al. Preliminary study of tetracycline resistance genes in Treponema pallidum. J. Glob. Antimicrob. Resist. 2017, 9, 1–2. [Google Scholar] [CrossRef]
- Workgroup, T.A.P. Prevalence of the 23S rRNA A2058G Point Mutation and Molecular Subtypes in Treponema pallidum in the United States, 2007 to 2009. Sex. Transm. Dis. 2012, 39, 794–798. [Google Scholar]
- Flasarová, M.; Pospíšilová, P.; Mikalová, L.; Vališová, Z.; Dastychová, E.; Strnadel, R.; Kuklová, I.; Woznicová, V.; Zákoucká, H.; Šmajs, D. Sequencing-based molecular typing of Treponema pallidum strains in the Czech Republic: All identified genotypes are related to the sequence of the SS14 strain. Acta Derm. Venereol. 2012, 92, 669–674. [Google Scholar] [CrossRef]
- Sanchez, A.; Mayslich, C.; Malet, I.; Grange, P.A.; Janier, M.; Saule, J.; Martinet, P.; Robert, J.-L.; Moulene, D.; Truchetet, F.; et al. Surveillance of Antibiotic Resistance Genes in Treponema Pallidum Subspecies Pallidum from Patients with Early Syphilis in France. Acta Derm. Venereol. 2020, 100, adv00221. [Google Scholar] [CrossRef]
- Khairullin, R.; Vorobyev, D.; Obukhov, A.; Kuular, U.-H.; Kubanova, A.; Kubanov, A.; Unemo, M. Syphilis epidemiology in 1994-2013, molecular epidemiological strain typing and determination of macrolide resistance in Treponema pallidum in 2013–2014 in Tuva Republic, Russia. APMIS Acta Pathol. Microbiol. Immunol. Scand. 2016, 124, 595–602. [Google Scholar] [CrossRef]
- Muldoon, E.G.; Walsh, A.; Crowley, B.; Mulcahy, F. Treponema pallidum azithromycin resistance in Dublin, Ireland. Sex. Transm. Dis. 2012, 39, 784–786. [Google Scholar] [CrossRef]
- Venter, J.M.E.; Müller, E.E.; Mahlangu, M.P.; Kularatne, R.S. Treponema pallidum Macrolide Resistance and Molecular Epidemiology in Southern Africa, 2008 to 2018. J. Clin. Microbiol. 2021, 59, e0238520. [Google Scholar] [CrossRef]
- Flores, J.A.; Vargas, S.K.; Leon, S.R.; Perez, D.G.; Ramos, L.B.; Chow, J.; Konda, K.A.; Calvo, G.M.; Salvatierra, H.J.; Klausner, J.D.; et al. Treponema pallidum pallidum Genotypes and Macrolide Resistance Status in Syphilitic Lesions among Patients at 2 Sexually Transmitted Infection Clinics in Lima, Peru. Sex. Transm. Dis. 2016, 43, 465–466. [Google Scholar] [CrossRef]
- Li, Z.; Hou, J.; Zheng, R.; Li, Z.; Wen, J.; Liu, D.; Liu, R.; Chu, T.; Liu, B.; Yu, G.; et al. Two mutations associated with macrolide resistance in Treponema pallidum in Shandong, China. J. Clin. Microbiol. 2013, 51, 4270–4271. [Google Scholar] [CrossRef] [Green Version]
- Grimes, M.; Sahi, S.K.; Godornes, B.C.; Tantalo, L.C.; Roberts, N.; Bostick, D.; Marra, C.M.; Lukehart, S.A. Two mutations associated with macrolide resistance in Treponema pallidum: Increasing prevalence and correlation with molecular strain type in Seattle, Washington. Sex. Transm. Dis. 2012, 39, 954–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cada Día, Más de 1 Millón de Personas Contraen una Infección de Transmisión Sexual Curable. Available online: https://www.who.int/es/news/item/06-06-2019-more-than-1-million-new-curable-sexually-transmitted-infections-every-day (accessed on 1 November 2022).
- National Overview. Available online: https://www.cdc.gov/std/statistics/2020/overview.htm (accessed on 1 November 2022).
- Chew Ng, R.A.; Samuel, M.C.; Lo, T.; Bernstein, K.T.; Aynalem, G.; Klausner, J.D.; Bolan, G. Sex, Drugs (Methamphetamines), and the Internet: Increasing Syphilis among Men Who Have Sex with Men in California, 2004–2008. Am. J. Public Health 2013, 103, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Marshall, B.M.; Levy, S.B. Food Animals and Antimicrobials: Impacts on Human Health. Clin. Microbiol. Rev. 2011, 24, 718–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matějková, P.; Flasarová, M.; Zákoucká, H.; Bořek, M.; Křemenová, S.; Arenberger, P.; Woznicová, V.; Weinstock, G.M.; Šmajs, D. Macrolide treatment failure in a case of secondary syphilis: A novel A2059G mutation in the 23S rRNA gene of Treponema pallidum subsp. pallidum. J. Med. Microbiol. 2009, 58, 832–836. [Google Scholar] [CrossRef]
- Ros-Vivancos, C.; González-Hernández, M.; Navarro-Gracia, J.F.; Sánchez-Payá, J.; González-Torga, A.; Portilla-Sogorb, J. Evolution of treatment of syphilis through history. Rev. Esp. Quimioter. Publ. Off. Soc. Esp. Quimioter. 2018, 31, 485–492. [Google Scholar]
- Stamm, L.V. Global Challenge of Antibiotic-Resistant Treponema pallidum. Antimicrob. Agents Chemother. 2010, 54, 583–589. [Google Scholar] [CrossRef] [Green Version]
- Stamm, L.V. Syphilis: Re-emergence of an old foe. Microb. Cell Graz Austria 2016, 3, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Kaul, R.; Kimani, J.; Nagelkerke, N.J.; Fonck, K.; Ngugi, E.N.; Keli, F.; MacDonald, K.S.; Maclean, I.W.; Bwayo, J.J.; Temmerman, M.; et al. Monthly antibiotic chemoprophylaxis and incidence of sexually transmitted infections and HIV-1 infection in Kenyan sex workers: A randomized controlled trial. JAMA 2004, 291, 2555–2562. [Google Scholar] [CrossRef]
- Bolan, R.K.; Beymer, M.R.; Weiss, R.E.; Flynn, R.P.; Leibowitz, A.A.; Klausner, J.D. Doxycycline prophylaxis to reduce incident syphilis among HIV-infected men who have sex with men who continue to engage in high-risk sex: A randomized, controlled pilot study. Sex. Transm. Dis. 2015, 42, 98–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, J.-M.; Charreau, I.; Chidiac, C.; Pialoux, G.; Cua, E.; Delaugerre, C.; Capitant, C.; Rojas-Castro, D.; Fonsart, J.; Bercot, B.; et al. Post-exposure prophylaxis with doxycycline to prevent sexually transmitted infections in men who have sex with men: An open-label randomised substudy of the ANRS IPERGAY trial. Lancet Infect. Dis. 2018, 18, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Marra, C.M.; Colina, A.P.; Godornes, C.; Tantalo, L.C.; Puray, M.; Centurion-Lara, A.; Lukehart, S.A. Antibiotic Selection May Contribute to Increases in Macrolide-Resistant Treponema pallidum. J. Infect. Dis. 2006, 194, 1771–1773. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Publication Year | Continent | Country | Recruiment Year | Sample Size (n) | Sex | Age Range or Median/Mean (Years) | MSM Population (n) | HIV Population (n) | Syphilis Molecular Detection (%) | A2058G Mutation (%) | A2059G Mutation (%) | Previous tx | Strain | Recruiting Place | Income Economies |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bourgeois G, 2021 [26] | Europe | France | 2018 | 119 | Both | NR | 6 | NR | 13.95 | 39 | NE | NO | NE | STI clinic | High |
| Mitchell SJ, 2006 [27] | America | USA | 2000–2004 | 154 | Men | 30.5–44 | 138 | 37 | 76.6 | NE | NE | Yes | NE | STI clinic | High |
| Read P, 2014 [28] | Oceania | Australia | 2004–2011 | 3037 | Men | 21–71 | 203 | 118 | 13.5 | 86 | NE | Yes | Yes | STI clinic | High |
| Fernández-Naval C, 2019 [29] | Europe | Spain | 2015 | 213 | Both | NR | 202 | NR | 61 | 99.1 | 0.9 | NR | 14d | STI clinic | High |
| Giacani L, 2018 [30] | Europe | Italy | 2016–2017 | 60 | W (n = 1); M (n = 59) | 18–70 | 52 | 21 | 88.3 | 98 | 2 | NR | 14d | STI clinic | High |
| Nishiki S, 2020 [31] | Asia | Japan | 2017–2018 | 482 | Both | <15–>60 | 34 | NR | 36.5 | 100 | 0 | Yes | 14d | STI clinic | High |
| Vann Damme K, 2009 [32] | Africa | Madagascar | 2000–2007 | 186 | Both | 18–53 | 4 | NR | 78.5 | 0 | NE | Yes | NE | STI clinic | Low |
| Wu H, 2012 [33] | Asia | China | 2009–2011 | 136 | W (n = 4); M (n = 132) | 19.6–57.9 | 109 | 93 | 55.3 | 0 | 0 | NO | 14f | HIV care clinic | Upper- middle |
| Noda AA, 2016 [12] | America | Cuba | 2012–2015 | 41 | M (n = 41) | 16–52 | 32 | 28 | 100 | 61 | 0 | Yes | 14f | General care clinic | Upper- middle |
| Lu H, 2015 [34] | Asia | China | 2007–2009 | 182 | W (n = 34); M (n = 75) | 39.9 Mean | NR | NR | 59.9 | 95.4 | NE | Yes | NE | STI clinic | Upper- middle |
| Chen XS, 2013 [35] | Asia | China | 2008–2011 | 391 | W (n = 50); M (n = 161) | 29–44 | 2 | 1 | 60.9 | 91.9 | NE | Yes | NE | STI clinic | Upper- middle |
| Tipple C, 2011 [36] | Europe | UK | 2006–2008 | 99 | Men | 24–54 | 17 | 11 | 19 | 91 | 8.3 | NR | 14d | STI clinic | High |
| Zhu B, 2016 [37] | Asia | China | 2012–2014 | 265 | W (37); M (141); n/d 87) | 17–85 | NR | 5 | 100 | 91 | NE | Yes | 14d | STI clinic | Upper- middle |
| Martin IE, 2009 [38] | America | Canada | 2007–2008 | 39 | W (n = 6); M (33) | 21–57 | NR | 1 | 97.4 | 100 | NE | NR | 14f | STI clinic | High |
| Müller EE, 2012 [39] | Africa | South Africa and Lesotho | 2005–2010 | 117 | M (n = 117) | NR | NR | NR | 85 | 1 | NE | Yes | 14d | STI clinic | Low |
| Vrbová E, 2019 [40] | Europe | Czech Republic | 2004–2017 | 675 | W (n = 25); M (n = 244); n/d (n = 406) | 0–71 | NR | NR | 41.6 | 53.7 | 4.4 | NR | NE | STI clinic | High |
| Liu D, 2021 [25] | Asia | China | 2016–2017 | 78 | W (n = 8); M (n = 41); n/d (n = 29) | 27–62 | NR | NR | 62.8 | 100 | 0 | NR | 16d | NR | Upper- middle |
| Martin IE, 2009 [38] | America | Canada | 2007–2008 | 68 | W (n = 21); M (n = 47) | 0–97.3 | 3 | NR | 50.6 | 36.8 | NE | NR | NE | STI clinic | High |
| Zondag HCA, 2020 [41] | Europe | Nederland | 2016 y 2017 | 135 | W (n = 1); M (n = 134) | 33–50 | 74 | 29 | 100 | 86 | 0 | Yes | 14d | Health Public Lab | High |
| Katz KA, 2010 [42] | America | USA | 2004–2007 | 74 | M (n = 69); n/d (n = 5) | 23–64 | NR | 30 | 93 | 71.2 | NE | Yes | 14d | STI clinic | High |
| Xiao Y, 2016 [43] | Asia | China | 2013–2015 | 2253 | W (n = 1243); M (n = 1010) | 16.1–82.5 | NR | NR | 20.2 | 97.5 | 0 | NR | 14d | STI clinic | Upper- middle |
| Kanai M, 2019 [44] | Asia | Japan | 2017 | 156 | W (n = 12); M (n = 61); n/d (n = 83) | NR | 25 | NR | 52.6 | 83.3 | 0 | NR | 14d | STI clinic | High |
| Shuel M, 2018 [45] | America | Canada | 2012–2016 | 354 | W (n = 14); M (n = 60); n/d (n = 280) | 1 month–70 years | NR | NR | 20.9 | 97.3 | 2.7 | NR | 14d | STI clinic | High |
| Mikalová L, 2017 [24] | Europe | Belgium | 2014–2015 | 72 | Both | 31–50 | NR | 72 | 40.3 | 65.5 | 0 | NR | 14j | STI clinic | High |
| Grillová L, 2014 [46] | Europe | Czech Republic | 2011–2013 | 188 | W (n = 22); M (n = 166) | 35.4 | 96 | 37 | 54.8 | 56 | 10.1 | NR | NE | STI clinic | High |
| Gallo Vaulet L, 2017 [47] | America | Argentina | 2006 y 2013 | 54 | W (n = 6); M (n = 48) | 17–66 | 27 | 12 | 76.9 | 9 | 4.7 | NR | 14d | General care clinic | Upper- middle |
| Martin IE, 2010 [48] | America | Canada | 2007–2009 | 374 | W (n = 146); M (n = 177); n/d (n = 51) | 0.1–97 | 7 | NR | 11.5 | 16.3 | NE | NR | 14d | General care clinic | High |
| Wu BR, 2014 [49] | Asia | China | 2009–2013 | 375 | W (n = 1); M (n = 371); n/d (n = 3) | 31.8 | 349 | 306 | 57.6 | 7 | 0 | NR | 14f | HIV care clinic | Upper- middle |
| Grillová L, 2019 [50] | America | Cuba | 2012–2017 | 83 | Both | 25–44 | 69 | 57 | 100 | 90.3 | NE | Yes | NE | STI clinic | Upper- middle |
| Xiao H, 2017 [51] | Asia | China | 2014–2015 | 183 | Both | NR | NR | NR | 93.4 | NE | NE | NR | NE | STI clinic | Upper- middle |
| Su JR, 2012 [52] | America | USA | 2007–2009 | 651 | W (n = 21); M (n = 118); n/d (n = 512) | 13–68 | 82 | 28 | 21.6 | 53.2 | NE | NR | 14d | STI clinic | High |
| Flasarová M, 2012 [53] | Europe | Czech Republic | 2004–2010 | 294 | W (n = 35); M (n = 156); n/d (n = 103) | 30.4 | NR | NR | 30.9 | 60.3 | 39.3 | NR | 14d | STI clinic | High |
| Sanchez A, 2020 [54] | Europe | France | 2010–2017 | 146 | W (n = 3); M (n = 143) | 21–71 | 115 | 39 | 100 | 85 | 0 | Yes | NE | STI clinic | High |
| Wu BR, 2014 [49] | Asia | China | 2009–2013 | 375 | W (n = 1); M (n = 371); n/d (n = 3) | NR | 349 | 306 | 57.6 | 7 | 0 | NR | NE | NR | Upper- middle |
| Khairullin R, 2016 [55] | Asia | Russia | 2013–2014 | 95 | W (n = 54); M (n = 41) | 15–80 | NR | 0 | 89.5 | 2.4 | NE | Yes | 14d | STI clinic | Upper- middle |
| Muldoon EG, 2012 [56] | Europe | Ireland | 2009–2010 | 92 | W (n = 4); M (n = 88) | 19–64 | 72 | NR | 31.5 | 93.1 | NE | NR | NE | STI clinic | High |
| Coelho EC, 2021 [23] | America | Brazil | 2015–2019 | 180 | W (180) | 23.5 | 0 | NR | 41.1 | 7.4 | 8.8 | Yes | NE | STI clinic | Upper- middle |
| Venter JME, 2021 [57] | Africa | Botswana, Zimbabwe, and South Africa | 2008–2018 | 135 | Both | 24–34 | NR | 46 | 100 | 22 | 0 | NR | 14d | STI clinic | Low |
| Flores JA, 2016 [58] | America | Peru | 2013–2014 | 26 | Both | NR | 26 | 12 | 69.2 | 0 | 0 | NR | 14d | STI clinic | Upper- middle |
| Li Z, 2013 [59] | Asia | China | 2010–2012 | 73 | Both | NR | NR | 0 | 90.4 | 92.4 | 7.6 | NR | NE | STI clinic | Upper- middle |
| Grimes M, 2012 [60] | America | USA | 2001–2010 | 129 | W (n = 2); M (n = 127) | NR | 125 | 112 | 100 | 62 | 1 | Yes | 14d | General care clinic | High |
| Study | Study Design | Selection (5) | Comparability (2) | Outcome (3) | Global Punctuation (10) | Interpretation |
|---|---|---|---|---|---|---|
| Bourgeois G, 2021 [26] | Cross-sectional | 4 | 0 | 3 | 7 | High |
| Mitchell SJ, 2006 [27] | Cross-sectional | 3 | 0 | 3 | 6 | Moderate |
| Read P, 2014 [28] | Cross-sectional | 3 | 0 | 3 | 6 | Moderate |
| Fernández-Naval C, 2019 [29] | Cross-sectional | 4 | 0 | 3 | 7 | High |
| Giacani L, 2018 [30] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
| Nishiki S, 2020 [31] | Cross-sectional | 4 | 2 | 2 | 8 | High |
| Damme K, 2009 [32] | Cross-sectional | 5 | 0 | 3 | 8 | High |
| Wu H, 2012 [33] | Cross-sectional | 4 | 0 | 3 | 7 | High |
| Noda AA, 2016 [12] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
| Lu H, 2015 [34] | Cross-sectional | 2 | 2 | 3 | 7 | High |
| Chen XS, 2013 [35] | Cross-sectional | 4 | 2 | 3 | 9 | High |
| Tipple C, 2011 [36] | Cross-sectional | 4 | 0 | 3 | 7 | High |
| Zhu B, 2016 [37] | Cross-sectional | 2 | 2 | 3 | 7 | High |
| Martin IE, 2009 [38] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
| Müller EE, 2012 [39] | Cross-sectional | 5 | 0 | 3 | 8 | High |
| Vrbová E, 2019 [40] | Cross-sectional | 4 | 2 | 3 | 9 | High |
| Liu D, 2021 [25] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
| Martin IE, 2009 [38] | Cross-sectional | 2 | 0 | 3 | 5 | Moderate |
| Zondag HCA, 2020 [41] | Cross-sectional | 2 | 0 | 3 | 5 | Moderate |
| Katz KA, 2010 [42] | Cross-sectional | 4 | 2 | 3 | 9 | High |
| Xiao Y, 2016 [43] | Cross-sectional | 2 | 0 | 3 | 5 | Moderate |
| Kanai M, 2019 [44] | Cross-sectional | 4 | 2 | 3 | 9 | High |
| Shuel M, 2018 [45] | Cross-sectional | 3 | 2 | 2 | 7 | High |
| Mikalová L, 2017 [24] | Cross-sectional | 3 | 2 | 2 | 7 | High |
| Grillová L, 2014 [46] | Cross-sectional | 3 | 2 | 3 | 8 | High |
| Gallo Vaulet L, 2017 [47] | Cross-sectional | 4 | 2 | 3 | 9 | High |
| Martin IE, 2010 [48] | Cross-sectional | 3 | 2 | 2 | 7 | High |
| Wu BR, 2014 [49] | Cross-sectional | 3 | 2 | 3 | 8 | High |
| Grillová L, 2019 [50] | Cross-sectional | 4 | 2 | 3 | 9 | High |
| Xiao H, 2017 [51] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
| Su JR, 2012 [52] | Cross-sectional | 3 | 2 | 3 | 8 | High |
| Flasarová M, 2012 [53] | Cross-sectional | 3 | 2 | 3 | 8 | High |
| Sanchez A, 2020 [54] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
| Wu BR, 2014 [49] | Cross-sectional | 3 | 0 | 2 | 5 | Moderate |
| Khairullin R, 2016 [55] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
| Muldoon EG, 2012 [56] | Cross-sectional | 3 | 0 | 2 | 5 | Moderate |
| Coelho EC, 2021 [23] | Cross-sectional | 4 | 2 | 3 | 9 | High |
| Venter JME, 2021 [57] | Cross-sectional | 4 | 0 | 3 | 7 | High |
| Flores JA, 2016 [58] | Cross-sectional | 3 | 0 | 2 | 5 | Moderate |
| Li Z, 2013 [59] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
| Grimes M, 2012 [60] | Cross-sectional | 4 | 0 | 2 | 6 | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orbe-Orihuela, Y.C.; Sánchez-Alemán, M.Á.; Hernández-Pliego, A.; Medina-García, C.V.; Vergara-Ortega, D.N. Syphilis as Re-Emerging Disease, Antibiotic Resistance, and Vulnerable Population: Global Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1546. https://doi.org/10.3390/pathogens11121546
Orbe-Orihuela YC, Sánchez-Alemán MÁ, Hernández-Pliego A, Medina-García CV, Vergara-Ortega DN. Syphilis as Re-Emerging Disease, Antibiotic Resistance, and Vulnerable Population: Global Systematic Review and Meta-Analysis. Pathogens. 2022; 11(12):1546. https://doi.org/10.3390/pathogens11121546
Chicago/Turabian StyleOrbe-Orihuela, Yaneth Citlalli, Miguel Ángel Sánchez-Alemán, Adriana Hernández-Pliego, Claudia Victoria Medina-García, and Dayana Nicté Vergara-Ortega. 2022. "Syphilis as Re-Emerging Disease, Antibiotic Resistance, and Vulnerable Population: Global Systematic Review and Meta-Analysis" Pathogens 11, no. 12: 1546. https://doi.org/10.3390/pathogens11121546