
Association of Fetal Lung Development Disorders with Adult Diseases: A Comprehensive Review
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Fetal Lung Development: An Overview
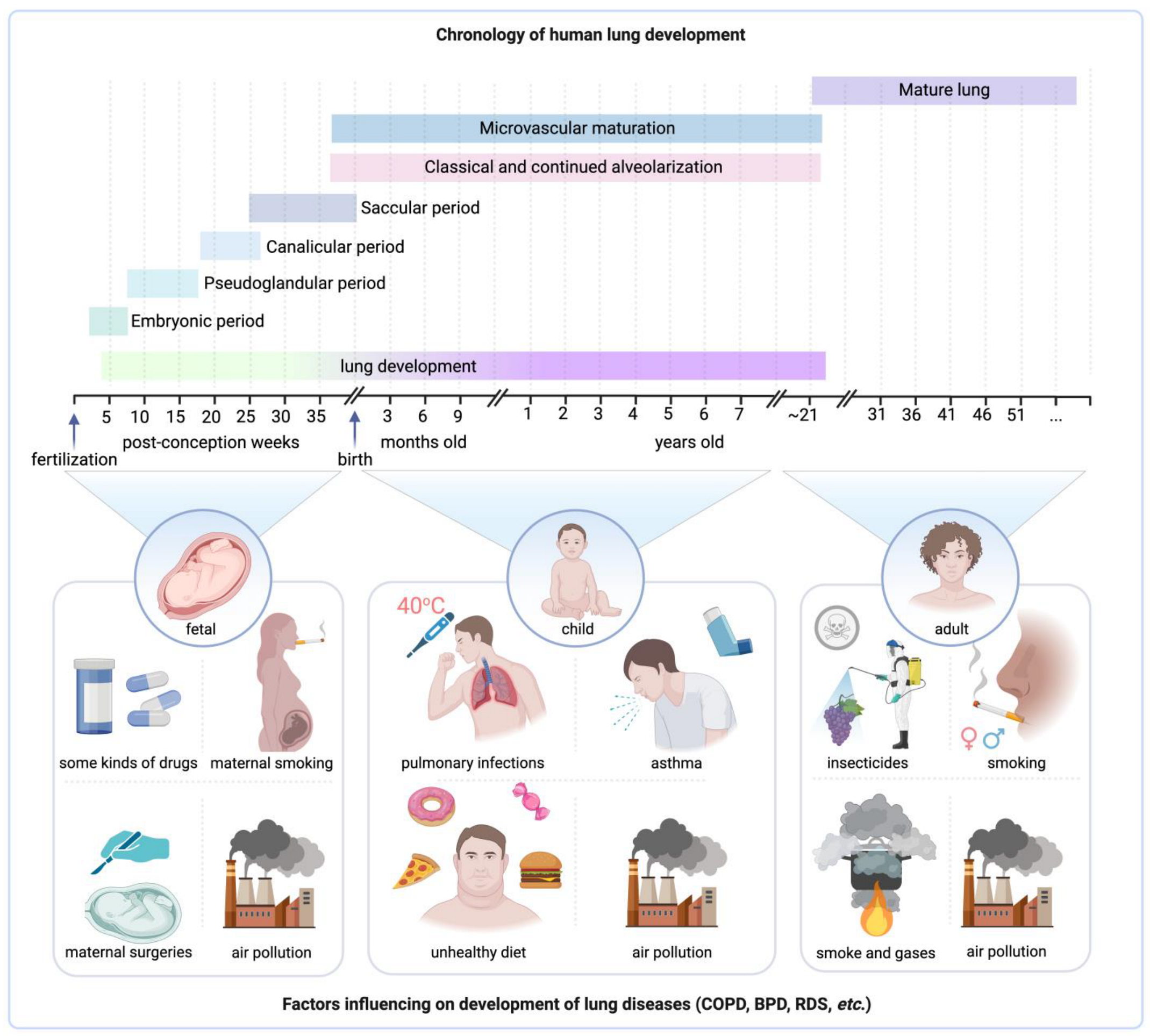
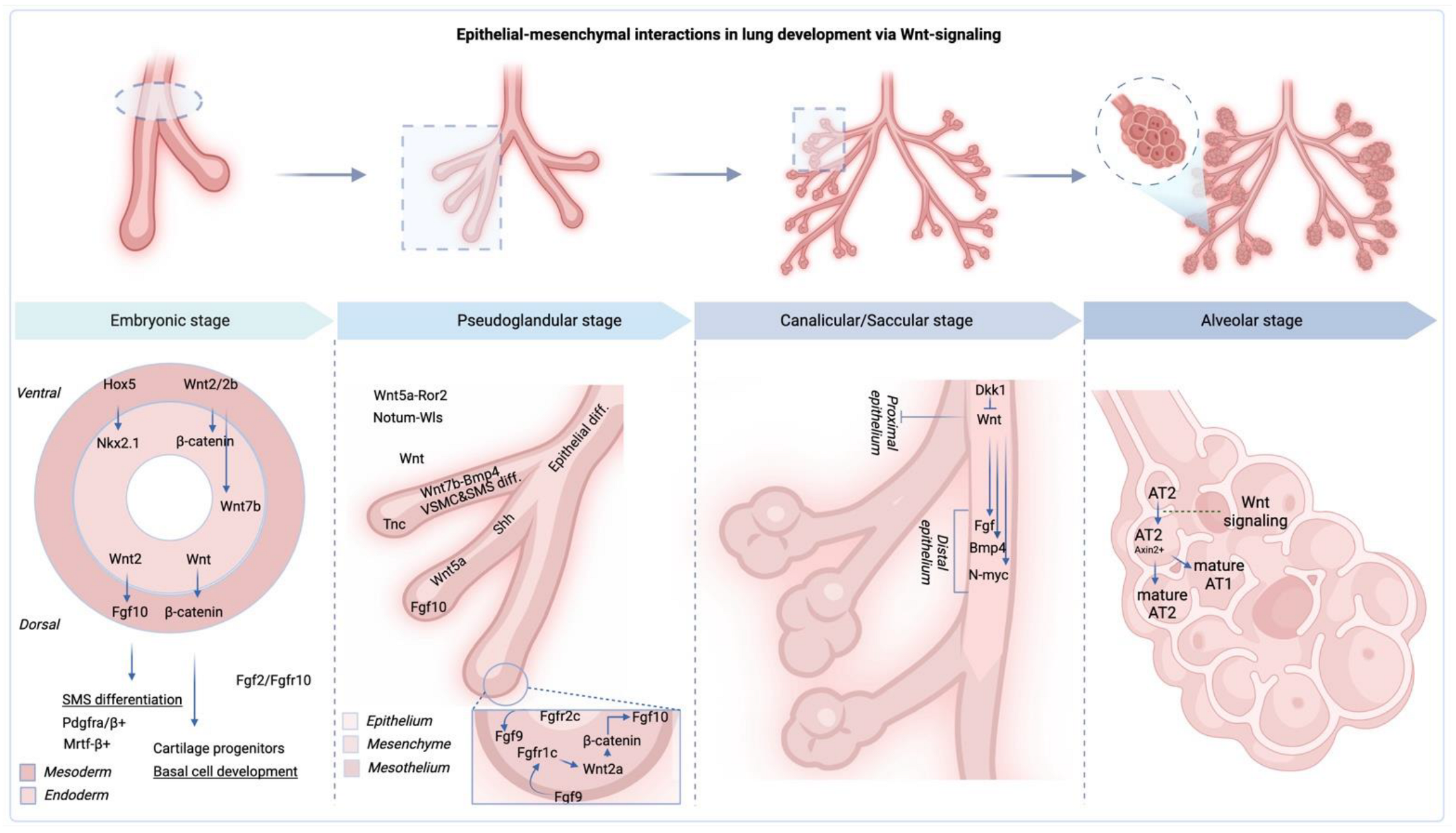
2.1. Stages of Fetal Lung Development
2.2. Key Factors Influencing Fetal Lung Maturation
2.3. Importance of Proper Fetal Lung Development for Postnatal Health
3. Fetal Lung Development Disorders
3.1. Respiratory Distress Syndrome (RDS)
3.2. Bronchopulmonary Dysplasia (BPD)
3.3. Congenital Diaphragmatic Hernia (CDH)
3.4. Other Fetal Lung Abnormalities
4. Linking Fetal Lung Development Disorders to Adult Diseases
4.1. Long-Term Consequences of Fetal Lung Development Disorders

4.2. Association of RDS with Adult Respiratory Diseases
4.3. Impact of BPD on Adult Lung Function and Respiratory Health
4.4. Relationship between CDH and Adult Respiratory Issues
5. Mechanisms Underlying Associations between Fetal Lung Development Disorders and Adult Respiratory Diseases
5.1. Epigenetic Modifications in Lung Development and Disease
5.2. The Impact of Environmental Factors during Intrauterine and Early Life Stages on Lung Development and Adult Health
6. Exploring Potential Therapeutic and Preventive Strategies in the Context of Fetal Lung Development Disorders and Adult Respiratory Health
7. Exploring Future Research Directions in the Domain of Fetal Lung Development Disorders and Associated Adult Diseases
8. Conclusions and Future Perspectives
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- He, P.; Lim, K.; Sun, D.; Pett, J.P.; Jeng, Q.; Polanski, K.; Dong, Z.; Bolt, L.; Richardson, L.; Mamanova, L.; et al. A Human Fetal Lung Cell Atlas Uncovers Proximal-Distal Gradients of Differentiation and Key Regulators of Epithelial Fates. Cell 2022, 185, 4841–4860.e25. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Feng, H.; Yi, H.; Pan, M.; Lin, L.; Zhang, Y.S.; Feng, Z.; Liang, W.; Cai, B.; Li, Q.; et al. Single-Cell RNA Sequencing Reveals the Developmental Program Underlying Proximal–Distal Patterning of the Human Lung at the Embryonic Stage. Cell Res. 2023, 33, 421–433. [Google Scholar] [CrossRef] [PubMed]
- Danopoulos, S.; Shiosaki, J.; Al Alam, D. FGF Signaling in Lung Development and Disease: Human Versus Mouse. Front. Genet. 2019, 10, 444859. [Google Scholar] [CrossRef] [PubMed]
- Loering, S.; Cameron, G.J.M.; Starkey, M.R.; Hansbro, P.M. Lung Development and Emerging Roles for Type 2 Immunity. J. Pathol. 2019, 247, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Andreas, A.; Maloy, A.; Nyunoya, T.; Zhang, Y.; Chandra, D. The FoxP1 Gene Regulates Lung Function, Production of Matrix Metalloproteinases and Inflammatory Mediators, and Viability of Lung Epithelia. Respir. Res. 2022, 23, 281. [Google Scholar] [CrossRef] [PubMed]
- Duong, T.E.; Wu, Y.; Sos, B.C.; Dong, W.; Limaye, S.; Rivier, L.H.; Myers, G.; Hagood, J.S.; Zhang, K. A Single-Cell Regulatory Map of Postnatal Lung Alveologenesis in Humans and Mice. Cell Genom. 2022, 2, 100108. [Google Scholar] [CrossRef] [PubMed]
- Saluzzo, S.; Gorki, A.D.; Rana, B.M.J.; Martins, R.; Scanlon, S.; Starkl, P.; Lakovits, K.; Hladik, A.; Korosec, A.; Sharif, O.; et al. First-Breath-Induced Type 2 Pathways Shape the Lung Immune Environment. Cell Rep. 2017, 18, 1893–1905. [Google Scholar] [CrossRef] [PubMed]
- RENESME, L.; Lesage, F.; Cook, D.P.; Zhong, S.; Hänninen, S.M.; Carpén, O.; Mižíková, I.; Thébaud, B. A Single-Cell Atlas of Human Fetal Lung Development between 14 and 19 Weeks of Gestation. Eur. Respir. J. 2022, 60, 145. [Google Scholar] [CrossRef]
- Hawkins, F.; Rankin, S.A.; Kotton, D.N.; Zorn, A.M. The Genetic Programs Regulating Embryonic Lung Development and Induced Pluripotent Stem Cell Differentiation. In Fetal and Neonatal Lung Development; Cambridge University Press: Cambridge, UK, 2016; pp. 1–21. [Google Scholar] [CrossRef]
- Cai, Q.; Luo, M.; Tang, Y.; Yu, M.; Yuan, F.; Gasser, G.N.; Liu, X.; Engelhardt, J.F. Sonic Hedgehog Signaling Is Essential for Pulmonary Ionocyte Specification in Human and Ferret Airway Epithelia. Am. J. Respir. Cell Mol. Biol. 2023, 69, 295–309. [Google Scholar] [CrossRef] [PubMed]
- Whitsett, J.A.; Wert, S.E.; Trapnell, B.C. Genetic Disorders Influencing Lung Formation and Function at Birth. Hum. Mol. Genet. 2004, 13 (Suppl. S2), R207–R215. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D. Overview of Lung Development in the Newborn Human. Neonatology 2017, 111, 398. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.D.; Alvira, C.M. Disrupted Lung Development and Bronchopulmonary Dysplasia: Opportunities for Lung Repair and Regeneration. Curr. Opin. Pediatr. 2014, 26, 306. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S. Maternal and Child Undernutrition: Consequences for Adult Health and Human Capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, C.M.; Saglani, S. Early-Life Respiratory Infections and Developmental Immunity Determine Lifelong Lung Health. Nat. Immunol. 2023, 24, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- Piedimonte, G.; Harford, T.J. Effects of Maternal−fetal Transmission of Viruses and Other Environmental Agents on Lung Development. Pediatr. Res. 2019, 87, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Thébaud, B.; Goss, K.N.; Laughon, M.; Whitsett, J.A.; Abman, S.H.; Steinhorn, R.H.; Aschner, J.L.; Davis, P.G.; McGrath-Morrow, S.A.; Soll, R.F.; et al. Bronchopulmonary Dysplasia. Nat. Rev. Dis. Primers 2019, 5, 78. [Google Scholar] [CrossRef] [PubMed]
- Bolton, C.E.; Bush, A.; Hurst, J.R.; Kotecha, S.; McGarvey, L. Lung Consequences in Adults Born Prematurely. Thorax 2015, 70, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Nikolić, M.Z.; Sun, D.; Rawlins, E.L. Human Lung Development: Recent Progress and New Challenges. Development 2018, 145, dev163485. [Google Scholar] [CrossRef] [PubMed]
- Rackley, C.R.; Stripp, B.R. Building and Maintaining the Epithelium of the Lung. J. Clin. Investig. 2012, 122, 2724–2730. [Google Scholar] [CrossRef] [PubMed]
- Schittny, J.C. Development of the Lung. Cell Tissue Res. 2017, 367, 427. [Google Scholar] [CrossRef] [PubMed]
- Macovei, T.; Sciuca, S.; Selevestru, R.; Eremciuc, R. The Impact of Teratogenic Factors in the Development of Pulmonary Hypoplasia in Children. Eur. Respir. J. 2013, 42, P1254. [Google Scholar]
- Kotecha, S.; Barbato, A.; Bush, A.; Claus, F.; Davenport, M.; Delacourt, C.; Deprest, J.; Eber, E.; Frenckner, B.; Greenough, A.; et al. Congenital Diaphragmatic Hernia. Eur. Respir. J. 2012, 39, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Lewis, L.; Sinha, I.; Kang, S.; Lim, J.; Losty, P. Long-Term Cardiorespiratory Outcomes in Congenital Diaphragmatic Hernia. Eur. Respir. J. 2022, 60, 3277. [Google Scholar] [CrossRef]
- Praprotnik, M.; Pavčnik, M.; Aldeco, M.; Srpčič, M.; Krivec, U. Lung Function in Survivors of Congenital Diaphragmatic Hernia at School Age. Eur. Respir. J. 2017, 50, PA1290. [Google Scholar] [CrossRef]
- Peetsold, M.G.; Heij, H.A.; Nagelkerke, A.F.; Ijsselstijn, H.; Tibboel, D.; Quanjer, P.H.; Gemke, R.J.B.J. Pulmonary Function and Exercise Capacity in Survivors of Congenital Diaphragmatic Hernia. Eur. Respir. J. 2009, 34, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Bellusci, S.; Warburton, D. Lung Development and Adult Lung Diseases. Chest 2007, 132, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Allinson, J.P.; Chaturvedi, N.; Wong, A.; Shah, I.; Donaldson, G.C.; Wedzicha, J.A.; Hardy, R. Early Childhood Lower Respiratory Tract Infection and Premature Adult Death from Respiratory Disease in Great Britain: A National Birth Cohort Study. Lancet 2023, 401, 1183–1193. [Google Scholar] [CrossRef] [PubMed]
- Stocks, J.; Hislop, A.; Sonnappa, S. Early Lung Development: Lifelong Effect on Respiratory Health and Disease. Lancet Respir. Med. 2013, 1, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Ubags, N.D.J.; Alejandre Alcazar, M.A.; Kallapur, S.G.; Knapp, S.; Lanone, S.; Lloyd, C.M.; Morty, R.E.; Pattaroni, C.; Reynaert, N.L.; Rottier, R.J.; et al. Early Origins of Lung Disease: Towards an Interdisciplinary Approach. Eur. Respir. Rev. 2020, 29, 200191. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and Attributable Health Burden of Chronic Respiratory Diseases, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585. [Google Scholar] [CrossRef] [PubMed]
- The Lancet GBD 2017: A Fragile World. Lancet 2018, 392, 1683. [CrossRef] [PubMed]
- Avena-Zampieri, C.L.; Hutter, J.; Rutherford, M.; Milan, A.; Hall, M.; Egloff, A.; Lloyd, D.F.A.; Nanda, S.; Greenough, A.; Story, L. Assessment of the Fetal Lungs in Utero. Am. J. Obstet. Gynecol. MFM 2022, 4, 100693. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.C.W.; Noble, P.B. Foetal Growth Restriction and Asthma: Airway Smooth Muscle Thickness Rather than Just Lung Size? Respirology 2020, 25, 889–891. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.F.; Frum, T.; Conchola, A.S.; Spence, J.R. Understanding Human Lung Development through In Vitro Model Systems. BioEssays 2020, 42, 2000006. [Google Scholar] [CrossRef] [PubMed]
- Hillman, N.H.; Lam, H.S. Respiratory Disorders in the Newborn. In Kendig’s Disorders of the Respiratory Tract in Children; Elsevier: Amsterdam, The Netherlands, 2019; pp. 338–366.e6. [Google Scholar] [CrossRef]
- Rehman, S.; Bacha, D. Embryology, Pulmonary. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Danopoulos, S.; Bhattacharya, S.; Mariani, T.J.; Al Alam, D. Transcriptional Characterisation of Human Lung Cells Identifies Novel Mesenchymal Lineage Markers. Eur. Respir. J. 2020, 55, 1900746. [Google Scholar] [CrossRef]
- Danopoulos, S.; Bhattacharya, S.; Thornton, M.; Grubbs, B.; Mariani, T.J.; Alam, D. Al Diversity in Mesenchymal Lineages during Early Human Lung Development. Eur. Respir. J. 2018, 52, PA1378. [Google Scholar] [CrossRef]
- Dagklis, T.; Tsakiridis, I.; Papazisis, G.; Athanasiadis, A. Efficacy and Safety of Corticosteroids’ Administration for Pulmonary Immaturity in Anticipated Preterm Delivery. Curr. Pharm. Des. 2021, 27, 3754–3761. [Google Scholar] [CrossRef] [PubMed]
- McGoldrick, E.; Stewart, F.; Parker, R.; Dalziel, S.R. Antenatal Corticosteroids for Accelerating Fetal Lung Maturation for Women at Risk of Preterm Birth. Cochrane Database Syst. Rev. 2020, 2021, CD004454. [Google Scholar] [CrossRef]
- Frey, U.; Usemann, J. Addressing the Complexity of Prenatal and Postnatal Environmental Exposures Affecting Childhood Lung Function. Lancet Planet Health 2019, 3, e51–e52. [Google Scholar] [CrossRef] [PubMed]
- Kuiper-Makris, C.; Zanetti, D.; Vohlen, C.; Fahle, L.; Müller, M.; Odenthal, M.; Felderhoff-Müser, U.; Dötsch, J.; Alejandre Alcazar, M.A. Mendelian Randomization and Experimental IUGR Reveal the Adverse Effect of Low Birth Weight on Lung Structure and Function. Sci. Rep. 2020, 10, 22395. [Google Scholar] [CrossRef] [PubMed]
- Abbas, G.; Shah, S.; Hanif, M.; Shah, A.; ur Rehman, A.; Tahir, S.; Nayab, K.; Asghar, A. The Frequency of Pulmonary Hypertension in Newborn with Intrauterine Growth Restriction. Sci. Rep. 2020, 10, 8064. [Google Scholar] [CrossRef] [PubMed]
- DenDekker, H.T.; Jaddoe, V.W.V.; Reiss, I.K.; De Jongste, J.C.; Duijts, L. Fetal and Infant Growth Patterns and Risk of Lower Lung Function and Asthma the Generation R Study. Am. J. Respir. Crit. Care Med. 2018, 197, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Bellusci, S.; Grindley, J.; Emoto, H.; Itoh, N.; Hogan, B.L.M. Fibroblast Growth Factor 10 (FGF10) and Branching Morphogenesis in the Embryonic Mouse Lung. Development 1997, 124, 4867–4878. [Google Scholar] [CrossRef] [PubMed]
- Tichelaar, J.W.; Lu, W.; Whitsett, J.A. Conditional Expression of Fibroblast Growth Factor-7 in the Developing and Mature Lung. J. Biol. Chem. 2000, 275, 11858–11864. [Google Scholar] [CrossRef] [PubMed]
- Hösgör, M.; IJzendoorn, Y.; Mooi, W.J.; Tibboel, D.; De Krijger, R.R. Thyroid Transcription Factor-1 Expression during Normal Human Lung Development and in Patients with Congenital Diaphragmatic Hernia. J. Pediatr. Surg. 2002, 37, 1258–1262. [Google Scholar] [CrossRef]
- Jo, H.S. Genetic Risk Factors Associated with Respiratory Distress Syndrome. Korean J. Pediatr. 2014, 57, 157. [Google Scholar] [CrossRef]
- Cole, F.S.; Hamvas, A.; Nogee, L.M. Genetic Disorders of Neonatal Respiratory Function. Pediatr. Res. 2001, 50, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Gower, W.A.; Nogee, L.M. Surfactant Dysfunction. Paediatr. Respir. Rev. 2011, 12, 223. [Google Scholar] [CrossRef] [PubMed]
- Herriges, M.; Morrisey, E.E. Lung Development: Orchestrating the Generation and Regeneration of a Complex Organ. Development 2014, 141, 502. [Google Scholar] [CrossRef]
- Kimura, Y.; Suzuki, T.; Kaneko, C.; Darnel, A.D.; Akahira, J.; Ebina, M.; Nukiwa, T.; Sasano, H. Expression of Androgen Receptor and 5alpha-Reductase Types 1 and 2 in Early Gestation Fetal Lung: A Possible Correlation with Branching Morphogenesis. Clin. Sci. 2003, 105, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Carey, M.A.; Card, J.W.; Voltz, J.W.; Arbes, S.J.; Germolec, D.R.; Korach, K.S.; Zeldin, D.C. It’s All about Sex: Gender, Lung Development and Lung Disease. Trends Endocrinol. Metab. 2007, 18, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Li, W.; Guo, Q.; Wang, Y.; Ma, L.; Zhang, X. Insulin-Like Growth Factor-1 Signaling in Lung Development and Inflammatory Lung Diseases. BioMed Res. Int. 2018, 2018, 6057589. [Google Scholar] [CrossRef] [PubMed]
- Bridges, J.P.; Sudha, P.; Lipps, D.; Wagner, A.; Guo, M.; YinaDu, X.; Brown, K.; Filuta, A.; Kitzmiller, J.; Stockman, C.; et al. Glucocorticoid Regulates Mesenchymal Cell Differentiation Required for Perinatal Lung Morphogenesis and Function. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2020, 319, L239–L255. [Google Scholar] [CrossRef] [PubMed]
- Habermehl, D.; Parkitna, J.R.; Kaden, S.; Brügger, B.; Wieland, F.; Gröne, H.J.; Schütz, G. Glucocorticoid Activity during Lung Maturation Is Essential in Mesenchymal and Less in Alveolar Epithelial Cells. Mol. Endocrinol. 2011, 25, 1280–1288. [Google Scholar] [CrossRef] [PubMed]
- Grier, D.G.; Halliday, H.L. Effects of Glucocorticoids on Fetal and Neonatal Lung Development. Treat. Respir. Med. 2004, 3, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Vyas, J.; Kotecha, S. Effects of Antenatal and Postnatal Corticosteroids on the Preterm Lung. Arch. Dis. Child. Fetal Neonatal Ed. 1997, 77, F147–F150. [Google Scholar] [CrossRef] [PubMed]
- Kemp, M.W.; Newnham, J.P.; Challis, J.G.; Jobe, A.H.; Stock, S.J. The Clinical Use of Corticosteroids in Pregnancy. Hum. Reprod. Update 2016, 22, 240–259. [Google Scholar] [CrossRef] [PubMed]
- Bolt, R.J.; van Weissenbruch, M.M.; Lafeber, H.N.; Delemarre-van de Waal, H.A. Glucocorticoids and Lung Development in the Fetus and Preterm Infant. Pediatr. Pulmonol. 2001, 32, 76–91. [Google Scholar] [CrossRef]
- McPherson, C.; Wambach, J.A. Prevention and Treatment of Respiratory Distress Syndrome in Preterm Neonates. Neonatal Netw. 2018, 37, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Hume, R.; Richard, K.; Kaptein, E.; Stanley, E.L.; Visser, T.J.; Coughtrie, M.W.H. Thyroid Hormone Metabolism and the Developing Human Lung. Biol. Neonate 2001, 80 (Suppl. S1), 18–21. [Google Scholar] [CrossRef] [PubMed]
- Rajatapiti, P.; Kester, M.H.A.; De Krijger, R.R.; Rottier, R.; Visser, T.J.; Tibboel, D. Expression of Glucocorticoid, Retinoid, and Thyroid Hormone Receptors during Human Lung Development. J. Clin. Endocrinol. Metab. 2005, 90, 4309–4314. [Google Scholar] [CrossRef] [PubMed]
- Banderali, G.; Martelli, A.; Landi, M.; Moretti, F.; Betti, F.; Radaelli, G.; Lassandro, C.; Verduci, E. Short and Long Term Health Effects of Parental Tobacco Smoking during Pregnancy and Lactation: A Descriptive Review. J. Transl. Med. 2015, 13, 327. [Google Scholar] [CrossRef] [PubMed]
- Rani, P.; Dhok, A. Effects of Pollution on Pregnancy and Infants. Cureus 2023, 15, e33906. [Google Scholar] [CrossRef] [PubMed]
- Kajekar, R. Environmental Factors and Developmental Outcomes in the Lung. Pharmacol. Ther. 2007, 114, 129–145. [Google Scholar] [CrossRef] [PubMed]
- Brabin, B.J.; Hakimi, M.; Pelletier, D. Role of Vitamin A in Lung Development. J. Nutr. 1995, 125, 1634S–1638S. [Google Scholar]
- Timoneda, J.; Rodríguez-Fernández, L.; Zaragozá, R.; Marín, M.P.; Cabezuelo, M.T.; Torres, L.; Viña, J.R.; Barber, T. Vitamin A Deficiency and the Lung. Nutrients 2018, 10, 1132. [Google Scholar] [CrossRef] [PubMed]
- Marquez, H.A.; Cardoso, W.V. Vitamin A-Retinoid Signaling in Pulmonary Development and Disease. Mol. Cell. Pediatr. 2016, 3, 28. [Google Scholar] [CrossRef] [PubMed]
- Checkley, W.; West, K.P.; Wise, R.A.; Baldwin, M.R.; Wu, L.; LeClerq, S.C.; Christian, P.; Katz, J.; Tielsch, J.M.; Khatry, S.; et al. Maternal Vitamin A Supplementation and Lung Function in Offspring. N. Engl. J. Med. 2010, 362, 1784–1794. [Google Scholar] [CrossRef] [PubMed]
- Vogel, E.R.; Britt, R.D.; Trinidad, M.C.; Faksh, A.; Martin, R.J.; MacFarlane, P.M.; Pabelick, C.M.; Prakash, Y.S. Perinatal Oxygen in the Developing Lung. Can. J. Physiol. Pharmacol. 2015, 93, 119. [Google Scholar] [CrossRef] [PubMed]
- Lakshminrusimha, S.; Saugstad, O.D. The Fetal Circulation, Pathophysiology of Hypoxemic Respiratory Failure and Pulmonary Hypertension in Neonates, and the Role of Oxygen Therapy. J. Perinatol. 2016, 36, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Domm, W.; Misra, R.S.; O’Reilly, M.A. Affect of Early Life Oxygen Exposure on Proper Lung Development and Response to Respiratory Viral Infections. Front. Med. 2015, 2, 1. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; Zhang, S.; Riddle, S.; Zhang, L.; Song, R.; Yue, D. Intrauterine Hypoxia and Epigenetic Programming in Lung Development and Disease. Biomedicines 2021, 9, 944. [Google Scholar] [CrossRef] [PubMed]
- Lomauro, A.; Aliverti, A. Sex Differences in Respiratory Function. Breathe 2018, 14, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Zosky, G.R.; Berry, L.J.; Elliot, J.G.; James, A.L.; Gorman, S.; Hart, P.H. Vitamin D Deficiency Causes Deficits in Lung Function and Alters Lung Structure. Am. J. Respir. Crit. Care Med. 2011, 183, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Korten, I.; Usemann, J.; Latzin, P. “Lung Sparing Growth”: Is the Lung Not Affected by Malnutrition? Eur. Respir. J. 2017, 49, 1700295. [Google Scholar] [CrossRef] [PubMed]
- Tyson, J.E.; Wright, L.L.; Oh, W.; Kennedy, K.A.; Mele, L.; Ehrenkranz, R.A.; Stoll, B.J.; Lemons, J.A.; Stevenson, D.K.; Bauer, C.R.; et al. Vitamin A Supplementation for Extremely-Low-Birth-Weight Infants. N. Engl. J. Med. 1999, 136, 124–125. [Google Scholar] [CrossRef] [PubMed]
- Moya, F. Preterm Nutrition and the Lung. World Rev. Nutr. Diet 2014, 110, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Arigliani, M.; Spinelli, A.M.; Liguoro, I.; Cogo, P. Nutrition and Lung Growth. Nutrients 2018, 10, 919. [Google Scholar] [CrossRef] [PubMed]
- Zeltner, T.B.; Burri, P.H. The Postnatal Development and Growth of the Human Lung. II. Morphology. Respir. Physiol. 1987, 67, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Hillman, N.H.; Kallapur, S.G.; Jobe, A.H. Physiology of Transition from Intrauterine to Extrauterine Life. Clin. Perinatol. 2012, 39, 769. [Google Scholar] [CrossRef] [PubMed]
- Gaultier, C. Postnatal Development of Lung Function. In Physiology of the Fetal and Neonatal Lung; Springer: Dordrecht, The Netherlands, 1987; pp. 139–154. [Google Scholar] [CrossRef]
- Gursoy, T.R.; Eyuboglu, T.S.; Aslan, A.T.; Karabulut, R.; Tastepe, I. Long-Term Follow-up of Children Diagnosed with Pulmonary Hypoplasia. Eur. Respir. J. 2021, 58, PA580. [Google Scholar] [CrossRef]
- Agustí, A.; Melén, E.; DeMeo, D.L.; Breyer-Kohansal, R.; Faner, R. Pathogenesis of Chronic Obstructive Pulmonary Disease: Understanding the Contributions of Gene-Environment Interactions across the Lifespan. Lancet Respir. Med. 2022, 10, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Mental Wellbeing and Lung Health. Breathe 2020, 16, 162ELF. [CrossRef] [PubMed]
- Lacagnina, S. The Developmental Origins of Health and Disease(DOHaD). Am. J. Lifestyle Med. 2020, 14, 47. [Google Scholar] [CrossRef]
- Ross, M.G.; Desai, M. Fetal Origins of Adult Health and Disease. In Genetic Disorders and the Fetus; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2021; pp. 214–239. [Google Scholar] [CrossRef]
- Mahoney, A.D.; Jain, L. Respiratory Disorders in Moderately Preterm, Late Preterm, and Early Term Infants. Clin. Perinatol. 2013, 40, 665–678. [Google Scholar] [CrossRef]
- Liu, J.; Sorantin, E. Neonatal Respiratory Distress Syndrome. In Neonatal Lung Ultrasonography; Springer: Dordrecht, The Netherlands, 2023; pp. 17–39. [Google Scholar] [CrossRef]
- Rubarth, L.B.; Quinn, J. Respiratory Development and Respiratory Distress Syndrome. Neonatal Netw. 2015, 34, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, A.S. The Most Frequent ABCA3 Nonsensemutation -p.Tyr1515* (Y1515X)Causing Lethal Neonatal Respiratoryfailure in a Term Neonate. Eur. Respir. J. 2017, 50, PA977. [Google Scholar] [CrossRef]
- Kinting, S.; Höppner, S.; Wittmann, T.; Schindlbeck, U.; Harfst, J.; Griese, M.; Zarbock, R. Rescue of Mutant ABCA3 by Small Molecular Correctors. Eur. Respir. J. 2017, 50, PA913. [Google Scholar] [CrossRef]
- Clarke, D.M.; Curtis, K.L.; Wendt, R.A.; Stapley, B.M.; Clark, E.T.; Beckett, N.; Campbell, K.M.; Arroyo, J.A.; Reynolds, P.R. Decreased Expression of Pulmonary Homeobox NKX2.1 and Surfactant Protein C in Developing Lungs That Over-Express Receptors for Advanced Glycation End-Products (RAGE). J. Dev. Biol. 2023, 11, 33. [Google Scholar] [CrossRef]
- Li, Y.; Wang, W.; Zhang, D. Maternal Diabetes Mellitus and Risk of Neonatal Respiratory Distress Syndrome: A Meta-Analysis. Acta Diabetol. 2019, 56, 729–740. [Google Scholar] [CrossRef] [PubMed]
- Mous, D.S.; Kool, H.M.; Wijnen, R.; Tibboel, D.; Rottier, R.J. Pulmonary Vascular Development in Congenital Diaphragmatic Hernia. Eur. Respir. Rev. 2018, 27, 170104. [Google Scholar] [CrossRef] [PubMed]
- Demir, O.F.; Hangul, M.; Kose, M. Congenital Lobar Emphysema: Diagnosis and Treatment Options. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 921. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, S.; Trovela, D.A.V. Congenital Lobar Emphysema. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Sashi Kumar, V.; Paul, V.K.; Sathasivam, K. Innovating Affordable Neonatal Care Equipment for Use at Scale. J. Perinatol. 2016, 36, S32–S36. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Fernandez, R.; Fox, G.F.; Goss, K.C.W.; Mactier, H.; Reynolds, P.; Sweet, D.G.; Roehr, C.C. Surfactant Replacement Therapy for Respiratory Distress Syndrome in Preterm Infants: United Kingdom National Consensus. Pediatr. Res. 2019, 86, 12–14. [Google Scholar] [CrossRef] [PubMed]
- Carlo, W.A.; Polin, R.A.; Papile, L.A.; Tan, R.; Kumar, P.; Benitz, W.; Eichenwald, E.; Cummings, J.; Baley, J. Respiratory Support in Preterm Infants at Birth. Pediatrics 2014, 133, 171–174. [Google Scholar] [CrossRef]
- Sakonidou, S.; Dhaliwal, J. The Management of Neonatal Respiratory Distress Syndrome in Preterm Infants (European Consensus Guidelines—2013 Update). Arch. Dis. Child. Educ. Pract. Ed. 2015, 100, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S.; Read, B.; Miller, M.; Da Silva, O. Impact of Catheter Choice on Procedural Success of Minimally Invasive Surfactant Therapy. Am. J. Perinatol. 2021, 40, 1202–1207. [Google Scholar] [CrossRef] [PubMed]
- Kakkilaya, V.; Gautham, K.S. Should Less Invasive Surfactant Administration (LISA) Become Routine Practice in US Neonatal Units? Pediatr. Res. 2022, 93, 1188–1198. [Google Scholar] [CrossRef] [PubMed]
- Escobar, V.; Soares, D.S.; Kreling, J.; Ferrari, L.S.L.; Felcar, J.M.; Camillo, C.A.M.; Probst, V.S. Influence of Time under Mechanical Ventilation on Bronchopulmonary Dysplasia Severity in Extremely Preterm Infants: A Pilot Study. BMC Pediatr. 2020, 20, 241. [Google Scholar] [CrossRef] [PubMed]
- Northway, W.H.; Moss, R.B.; Carlisle, K.B.; Parker, B.R.; Popp, R.L.; Pitlick, P.T.; Eichler, I.; Lamm, R.L.; Brown, B.W. Late Pulmonary Sequelae of Bronchopulmonary Dysplasia. N. Engl. J. Med. 1990, 323, 1793–1799. [Google Scholar] [CrossRef] [PubMed]
- Gough, A.; Linden, M.; Spence, D.; Patterson, C.C.; Halliday, H.L.; McGarvey, L.P.A. Impaired Lung Function and Health Status in Adult Survivors of Bronchopulmonary Dysplasia. Eur. Respir. J. 2014, 43, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Pasha, A.B.; Chen, X.Q.; Zhou, G.P. Bronchopulmonary Dysplasia: Pathogenesis and Treatment. Exp. Ther. Med. 2018, 16, 4315. [Google Scholar] [CrossRef] [PubMed]
- Zani, A.; Chung, W.K.; Deprest, J.; Harting, M.T.; Jancelewicz, T.; Kunisaki, S.M.; Patel, N.; Antounians, L.; Puligandla, P.S.; Keijzer, R. Congenital Diaphragmatic Hernia. Nat. Rev. Dis. Primers 2022, 8, 37. [Google Scholar] [CrossRef] [PubMed]
- Greenough, A.; Ali, K. Outcome of Infants with Right versus Left Sided Congenital Diaphragmatic Hernia. Eur. Respir. J. 2017, 50, PA2072. [Google Scholar] [CrossRef]
- Adaikalam, S.A.; Higano, N.S.; Tkach, J.A.; Yen Lim, F.; Haberman, B.; Woods, J.C.; Kingma, P.S. Neonatal Lung Growth in Congenital Diaphragmatic Hernia: Evaluation of Lung Density and Mass by Pulmonary MRI. Pediatr. Res. 2019, 86, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Puligandla, P.S.; Skarsgard, E.D.; Offringa, M.; Adatia, I.; Baird, R.; Bailey, J.A.M.; Brindle, M.; Chiu, P.; Cogswell, A.; Dakshinamurti, S.; et al. Diagnosis and Management of Congenital Diaphragmatic Hernia: A Clinical Practice Guideline. CMAJ 2018, 190, E103–E112. [Google Scholar] [PubMed]
- Dahl, M.J.; Lavizzari, A.; Davis, J.W.; Noble, P.B.; Dellacà, R.; Pillow, J.J. Impact of Fetal Treatments for Congenital Diaphragmatic Hernia on Lung Development. Anat. Rec. 2022; Epub ahead of printing. [Google Scholar] [CrossRef]
- Greenough, A. Management of Infants with Congenital Diaphragmatic Hernia and Pulmonary Hypertension—One Size Does Not Fit All. Pediatr. Res. 2023, 93, 1795–1796. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, G.; MacArthur, K.; Pollock, J.C. Congenital Lung Malformations—Antenatal and Postnatal Evaluation and Management. Eur. J. Cardio-Thorac. Surg. 2005, 27, 45–52. [Google Scholar] [CrossRef]
- Belcher, E.; Lawson, M.H.; Nicholson, A.G.; Davison, A.; Goldstraw, P. Congenital Cystic Adenomatoid Malformation Presenting as In-Flight Systemic Air Embolisation. Eur. Respir. J. 2007, 30, 801–804. [Google Scholar] [CrossRef] [PubMed]
- Ou, J.; Lei, X.; Fu, Z.; Huang, Y.; Liu, E.; Luo, Z.; Peng, D. Pulmonary Sequestration in Children: A Clinical Analysis of 48 Cases. Int. J. Clin. Exp. Med. 2014, 7, 1355. [Google Scholar] [PubMed]
- Wu, A.; Mukhtar-Yola, M.; Luch, S.; John, S.; Adhikari, B.R.; Bakker, C.; Slusher, T.; Bjorklund, A.; Winter, J.; Ezeaka, C. Innovations and Adaptations in Neonatal and Pediatric Respiratory Care for Resource Constrained Settings. Front. Pediatr. 2022, 10, 954975. [Google Scholar] [CrossRef] [PubMed]
- Postma, D.S.; Bush, A.; Van Den Berge, M. Risk Factors and Early Origins of Chronic Obstructive Pulmonary Disease. Lancet 2015, 385, 899–909. [Google Scholar] [CrossRef] [PubMed]
- Pike, K.; Jane Pillow, J.; Lucas, J.S. Long Term Respiratory Consequences of Intrauterine Growth Restriction. Semin. Fetal Neonatal Med. 2012, 17, 92–98. [Google Scholar] [CrossRef]
- Ward, S.L.; Turpin, A.; Spicer, A.C.; Treadwell, M.J.; Church, G.D.; Flori, H.R. Long Term Pulmonary Function and Quality of Life in Children after Acute Respiratory Distress Syndrome: A Feasibility Investigation. Pediatr. Crit. Care Med. 2017, 18, e48. [Google Scholar] [CrossRef] [PubMed]
- Steiner, L.; Diesner, S.C.; Voitl, P. Risk of Infection in the First Year of Life in Preterm Children: An Austrian Observational Study. PLoS ONE 2019, 14, e0224766. [Google Scholar] [CrossRef] [PubMed]
- Momtazmanesh, S.; Moghaddam, S.S.; Ghamari, S.H.; Rad, E.M.; Rezaei, N.; Shobeiri, P.; Aali, A.; Abbasi-Kangevari, M.; Abbasi-Kangevari, Z.; Abdelmasseh, M.; et al. Global Burden of Chronic Respiratory Diseases and Risk Factors, 1990–2019: An Update from the Global Burden of Disease Study 2019. eClinicalMedicine 2023, 59, 101936. [Google Scholar] [CrossRef]
- Beam, A.L.; Fried, I.; Palmer, N.; Agniel, D.; Brat, G.; Fox, K.; Kohane, I.; Sinaiko, A.; Zupancic, J.A.F.; Armstrong, J. Estimates of Healthcare Spending for Preterm and Low-Birthweight Infants in a Commercially Insured Population: 2008–2016. J. Perinatol. 2020, 40, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.E.; Jang, H.; Han, J.H.; Park, J.; Kim, S.Y.; Kim, Y.H.; Eun, H.S.; Lee, S.M.; Park, K.I.; Sohn, M.H.; et al. Association between Bronchopulmonary Dysplasia and Early Respiratory Morbidity in Children with Respiratory Distress Syndrome: A Case–Control Study Using Nationwide Data. Sci. Rep. 2022, 12, 7578. [Google Scholar] [CrossRef] [PubMed]
- Yamoto, M.; Nagata, K.; Terui, K.; Hayakawa, M.; Okuyama, H.; Amari, S.; Yokoi, A.; Masumoto, K.; Okazaki, T.; Inamura, N.; et al. Long-Term Outcomes of Congenital Diaphragmatic Hernia: Report of a Multicenter Study in Japan. Children 2022, 9, 856. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.C.-H.; Ma, S. The Role of Surfactant in Respiratory Distress Syndrome. Open Respir. Med. J. 2012, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Soll, R.; Morley, C.J. Prophylactic versus Selective Use of Surfactant in Preventing Morbidity and Mortality in Preterm Infants. Cochrane Database Syst. Rev. 2001, CD000510. [Google Scholar] [CrossRef]
- Courtney, S.E.; Long, W.; McMillan, D.; Walter, D.; Thompson, T.; Sauve, R.; Conway, B.; Bard, H. Double-Blind 1-Year Follow-up of 1540 Infants with Respiratory Distress Syndrome Randomized to Rescue Treatment with Two Doses of Synthetic Surfactant or Air in Four Clinical Trials. J. Pediatr. 1995, 126, S43–S52. [Google Scholar] [CrossRef] [PubMed]
- Sauve, R.; Long, W.; Vincer, M.; Bard, H.; Derleth, D.; Stevenson, D.; Pauly, T.; Robertson, C. Outcome at 1-Year Adjusted Age of 957 Infants Weighing More than 1250 Grams with Respiratory Distress Syndrome Randomized to Receive Synthetic Surfactant or Air Placebo. American and Canadian Exosurf Neonatal Study Groups. J. Pediatr. 1995, 126, S75–S80. [Google Scholar] [CrossRef]
- Ainsworth, S.B.; Milligan, D.W. Surfactant Therapy for Respiratory Distress Syndrome in Premature Neonates. Am. J. Respir. Med. 2012, 1, 417–433. [Google Scholar] [CrossRef]
- Wong, P.M.; Lees, A.N.; Louw, J.; Lee, F.Y.; French, N.; Gain, K.; Murray, C.P.; Wilson, A.; Chambers, D.C. Emphysema in Young Adult Survivors of Moderate-to-Severe Bronchopulmonary Dysplasia. Eur. Respir. J. 2008, 32, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Narang, I.; Rosenthal, M.; Cremonesini, D.; Silverman, M.; Bush, A. Longitudinal Evaluation of Airway Function 21 Years after Preterm Birth. Am. J. Respir. Crit. Care Med. 2008, 178, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, T.; Skadberg, B.T.; Eide, G.E.; Røksund, O.D.; Carlsen, K.H.; Bakke, P. Pulmonary Outcome in Adolescents of Extreme Preterm Birth: A Regional Cohort Study. Acta Paediatr. 2004, 93, 1294–1300. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.W.; Faber, B.; Callanan, C.; Freezer, N.; Ford, G.W.; Davis, N.M. Bronchopulmonary Dysplasia in Very Low Birth Weight Subjects and Lung Function in Late Adolescence. Pediatrics 2006, 118, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Cousins, M.; Hart, K.; Gallacher, D.; Palomino, M.A.; Kotecha, S. Long-term respiratory outcomes following preterm birth. Rev. Méd. Clín. Condes 2018, 29, 87–97. [Google Scholar] [CrossRef]
- Bhandari, A.; McGrath-Morrow, S. Long-Term Pulmonary Outcomes of Patients with Bronchopulmonary Dysplasia. Semin. Perinatol. 2013, 37, 132–137. [Google Scholar] [CrossRef]
- Homan, T.D.; Nayak, R.P. Short- and Long-Term Complications of Bronchopulmonary Dysplasia. Respir. Care 2021, 66, 1618–1629. [Google Scholar] [CrossRef] [PubMed]
- Principi, N.; Di Pietro, G.M.; Esposito, S. Bronchopulmonary Dysplasia: Clinical Aspects and Preventive and Therapeutic Strategies. J. Transl. Med. 2018, 16, 36. [Google Scholar] [CrossRef] [PubMed]
- Perrone, S.; Manti, S.; Buttarelli, L.; Petrolini, C.; Boscarino, G.; Filonzi, L.; Gitto, E.; Esposito, S.M.R.; Nonnis Marzano, F. Vascular Endothelial Growth Factor as Molecular Target for Bronchopulmonary Dysplasia Prevention in Very Low Birth Weight Infants. Int. J. Mol. Sci. 2023, 24, 2729. [Google Scholar] [CrossRef] [PubMed]
- Omar, S.A.; Abdul-Hafez, A.; Ibrahim, S.; Pillai, N.; Abdulmageed, M.; Thiruvenkataramani, R.P.; Mohamed, T.; Madhukar, B.V.; Uhal, B.D. Stem-Cell Therapy for Bronchopulmonary Dysplasia (BPD) in Newborns. Cells 2022, 11, 1275. [Google Scholar] [CrossRef] [PubMed]
- Simones, A.A.; Beisang, D.J.; Panoskaltsis-Mortari, A.; Roberts, K.D. Mesenchymal Stem Cells in the Pathogenesis and Treatment of Bronchopulmonary Dysplasia: A Clinical Review. Pediatr. Res. 2017, 83, 308–317. [Google Scholar] [CrossRef]
- Rocha, G.; Guimarães, H.; Pereira-Da-silva, L. The Role of Nutrition in the Prevention and Management of Bronchopulmonary Dysplasia: A Literature Review and Clinical Approach. Int. J. Environ. Res. Public Health 2021, 18, 6245. [Google Scholar] [CrossRef] [PubMed]
- Schulzke, S.M.; Pillow, J.J. The Management of Evolving Bronchopulmonary Dysplasia. Paediatr. Respir. Rev. 2010, 11, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Durham, A.L.; Adcock, I.M. Basic Science: Epigenetic Programming and the Respiratory System. Breathe 2013, 9, 278–288. [Google Scholar] [CrossRef]
- Wrede, D.; Bordak, M.; Abraham, Y.; Mehedi, M. Pulmonary Pathogen-Induced Epigenetic Modifications. Epigenomes 2023, 7, 13. [Google Scholar] [CrossRef]
- Peetsold, M.G.; Heij, H.A.; Kneepkens, C.M.F.; Nagelkerke, A.F.; Huisman, J.; Gemke, R.J.B.J. The Long-Term Follow-up of Patients with a Congenital Diaphragmatic Hernia: A Broad Spectrum of Morbidity. Pediatr. Surg. Int. 2009, 25, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.S.; Harting, M.T. Congenital Diaphragmatic Hernia-Associated Pulmonary Hypertension. Semin. Perinatol. 2020, 44, 151167. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.E.; Pober, B.R.; Adatia, I. Congenital Diaphragmatic Hernia and Associated Cardiovascular Malformations: Type, Frequency, and Impact on Management. Am. J. Med. Genet. C Semin. Med. Genet. 2007, 145C, 201. [Google Scholar] [CrossRef] [PubMed]
- Burgos, C.M.; Modée, A.; Öst, E.; Frenckner, B. Addressing the Causes of Late Mortality in Infants with Congenital Diaphragmatic Hernia. J. Pediatr. Surg. 2017, 52, 526–529. [Google Scholar] [CrossRef] [PubMed]
- Hollinger, L.E.; Buchmiller, T.L. Long Term Follow-up in Congenital Diaphragmatic Hernia. Semin. Perinatol. 2020, 44, 151171. [Google Scholar] [CrossRef] [PubMed]
- Tovar, J.A. Congenital Diaphragmatic Hernia. Orphanet J. Rare Dis. 2012, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Sluiter, I.; van de Ven, C.P.; Wijnen, R.M.H.; Tibboel, D. Congenital Diaphragmatic Hernia: Still a Moving Target. Semin. Fetal Neonatal Med. 2011, 16, 139–144. [Google Scholar] [CrossRef]
- Okuyama, H.; Kitano, Y.; Saito, M.; Usui, N.; Morikawa, N.; Masumoto, K.; Takayasu, H.; Nakamura, T.; Ishikawa, H.; Kawataki, M.; et al. The Japanese Experience with Prenatally Diagnosed Congenital Diaphragmatic Hernia Based on a Multi-Institutional Review. Pediatr. Surg. Int. 2011, 27, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Rocha, G.; Azevedo, I.; Pinto, J.C.; Guimarães, H. Follow-up of the Survivors of Congenital Diaphragmatic Hernia. Early Hum. Dev. 2012, 88, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Jancelewicz, T.; Chiang, M.; Oliveira, C.; Chiu, P.P. Late Surgical Outcomes among Congenital Diaphragmatic Hernia (CDH) Patients: Why Long-Term Follow-up with Surgeons Is Recommended. J. Pediatr. Surg. 2013, 48, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Zhang, X.L.; Ahmad, A. Epigenetic Regulation of Pulmonary Inflammation. Semin. Cell Dev. Biol. 2024, 154, 346–354. [Google Scholar] [CrossRef]
- Mijač, S.; Banić, I.; Genc, A.M.; Lipej, M.; Turkalj, M. The Effects of Environmental Exposure on Epigenetic Modifications in Allergic Diseases. Medicina 2024, 60, 110. [Google Scholar] [CrossRef] [PubMed]
- Breton, C.V.; Landon, R.; Kahn, L.G.; Enlow, M.B.; Peterson, A.K.; Bastain, T.; Braun, J.; Comstock, S.S.; Duarte, C.S.; Hipwell, A.; et al. Exploring the Evidence for Epigenetic Regulation of Environmental Influences on Child Health across Generations. Commun. Biol. 2021, 4, 769. [Google Scholar] [CrossRef] [PubMed]
- Hagood, J.S. Beyond the Genome: Epigenetic Mechanisms in Lung Remodeling. Physiology 2014, 29, 177. [Google Scholar] [CrossRef] [PubMed]
- Benincasa, G.; DeMeo, D.L.; Glass, K.; Silverman, E.K.; Napoli, C. Epigenetics and Pulmonary Diseases in the Horizon of Precision Medicine: A Review. Eur. Respir. J. 2021, 57, 2003406. [Google Scholar] [CrossRef] [PubMed]
- Joss-Moore, L.A.; Lane, R.H.; Albertine, K.H. Epigenetic Contributions to the Developmental Origins of Adult Lung Disease. Biochem. Cell Biol. 2015, 93, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Mei, Q.; Liu, Z.; Zuo, H.; Yang, Z.; Qu, J. Idiopathic Pulmonary Fibrosis: An Update on Pathogenesis. Front. Pharmacol. 2021, 12, 797292. [Google Scholar] [CrossRef] [PubMed]
- Korfei, M.; Mahavadi, P.; Guenther, A. Targeting Histone Deacetylases in Idiopathic Pulmonary Fibrosis: A Future Therapeutic Option. Cells 2022, 11, 1626. [Google Scholar] [CrossRef] [PubMed]
- Bartczak, K.; Białas, A.J.; Kotecki, M.J.; Górski, P.; Piotrowski, W.J. More than a Genetic Code: Epigenetics of Lung Fibrosis. Mol. Diagn. Ther. 2020, 24, 665–681. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Lu, C.; Norbäck, D.; Bornehag, C.G.; Zhang, Y.; Liu, W.; Yuan, H.; Sundell, J. Early Life Exposure to Ambient Air Pollution and Childhood Asthma in China. Environ. Res. 2015, 143, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Kabesch, M.; Michel, S.; Tost, J. Epigenetic Mechanisms and the Relationship to Childhood Asthma. Eur. Respir. J. 2010, 36, 950–961. [Google Scholar] [CrossRef]
- Liu, H.; Yin, T.; Yan, W.; Si, R.; Wang, B.; Chen, M.; Li, F.; Wang, Q.; Tao, L. Dysregulation of MicroRNA-214 and PTEN Contributes to the Pathogenesis of Hypoxic Pulmonary Hypertension. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1781–1791. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cho, H.Y.; Campbell, M.R.; Panduri, V.; Coviello, S.; Caballero, M.T.; Sambandan, D.; Kleeberger, S.R.; Polack, F.P.; Ofman, G.; et al. Epigenome-Wide Association Study of Bronchopulmonary Dysplasia in Preterm Infants: Results from the Discovery-BPD Program. Clin. Epigenet. 2022, 14, 57. [Google Scholar] [CrossRef]
- Gibbs, K.; Collaco, J.M.; McGrath-Morrow, S.A. Impact of Tobacco Smoke and Nicotine Exposure on Lung Development. Chest 2016, 149, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Landau, L.I. Tobacco Smoke Exposure and Tracking of Lung Function into Adult Life. Paediatr. Respir. Rev. 2008, 9, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Den Dekker, H.T.; Sonnenschein-Van Der Voort, A.M.M.; De Jongste, J.C.; Reiss, I.K.; Hofman, A.; Jaddoe, V.W.V.; Duijts, L. Tobacco Smoke Exposure, Airway Resistance, and Asthma in School-Age Children: The Generation R Study. Chest 2015, 148, 607–617. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, C.T.; Spindel, E.R. Pulmonary Effects of Maternal Smoking on the Fetus and Child: Effects on Lung Development, Respiratory Morbidities, and Life Long Lung Health. Paediatr. Respir. Rev. 2017, 21, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Grant, T.; Brigham, E.P.; McCormack, M.C. Childhood Origins of Adult Lung Disease as Opportunities for Prevention. J. Allergy Clin. Immunol. Pract. 2020, 8, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Spindel, E.R.; McEvoy, C.T. The Role of Nicotine in the Effects of Maternal Smoking during Pregnancy on Lung Development and Childhood Respiratory Disease. Implications for Dangers of E-Cigarettes. Am. J. Respir. Crit. Care Med. 2016, 193, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Burke, H.; Leonardi-Bee, J.; Hashim, A.; Pine-Abata, H.; Chen, Y.; Cook, D.G.; Britton, J.R.; McKeever, T.M. Prenatal and Passive Smoke Exposure and Incidence of Asthma and Wheeze: Systematic Review and Meta-Analysis. Pediatrics 2012, 129, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Neuman, Å.; Hohmann, C.; Orsini, N.; Pershagen, G.; Eller, E.; Kjaer, H.F.; Gehring, U.; Granell, R.; Henderson, J.; Heinrich, J.; et al. Maternal Smoking in Pregnancy and Asthma in Preschool Children: A Pooled Analysis of Eight Birth Cohorts. Am. J. Respir. Crit. Care Med. 2012, 186, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Hayatbakhsh, M.R.; Sadasivam, S.; Mamun, A.A.; Najman, J.M.; Williams, G.M.; O’Callaghan, M.J. Maternal Smoking during and after Pregnancy and Lung Function in Early Adulthood: A Prospective Study. Thorax 2009, 64, 810–814. [Google Scholar] [CrossRef] [PubMed]
- Lødrup Carlsen, K.C.; Jaakkola, J.J.K.; Nafstad, P.; Carlsen, K.H. In Utero Exposure to Cigarette Smoking Influences Lung Function at Birth. Eur. Respir. J. 1997, 10, 1774–1779. [Google Scholar] [CrossRef] [PubMed]
- Kauffmann, F.; Tager, I.B.; Mũoz, A.; Speizer, F.E. Familial Factors Related to Lung Function in Children Aged 6-10 Years. Results from the PAARC Epidemiologic Study. Am. J. Epidemiol. 1989, 129, 1289–1299. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.; Trump, S.; Ishaque, N.; Thürmann, L.; Gu, L.; Bauer, M.; Bieg, M.; Gu, Z.; Weichenhan, D.; Mallm, J.-P.; et al. Environment-Induced Epigenetic Reprogramming in Genomic Regulatory Elements in Smoking Mothers and Their Children. Mol. Syst. Biol. 2016, 12, 861. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Sundquist, J.; Winkleby, M.A.; Sundquist, K. Gestational Age at Birth and Mortality from Infancy into Mid-Adulthood: A National Cohort Study. Lancet Child Adolesc. Health 2019, 3, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Mu, X.; Deng, L.; Aili, F.; Pu, E.; Tang, T.; Kong, X. The Etiologic Origins for Chronic Obstructive Pulmonary Disease. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1139–1158. [Google Scholar] [CrossRef] [PubMed]
- Cosín-Tomás, M.; Bustamante, M.; Sunyer, J. Epigenetic Association Studies at Birth and the Origin of Lung Function Development. Eur. Respir. J. 2021, 57, 2100109. [Google Scholar] [CrossRef]
- Mocelin, H.T.; Fischer, G.B.; Bush, A. Adverse Early-Life Environmental Exposures and Their Repercussions on Adult Respiratory Health. J. Pediatr. 2022, 98 (Suppl. S1), S86–S95. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Chen, Z.; Zhou, L.F.; Huang, S.X. Air Pollutants and Early Origins of Respiratory Diseases. Chronic Dis. Transl. Med. 2018, 4, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Gruzieva, O.; Jeong, A.; He, S.; Yu, Z.; de Bont, J.; Pinho, M.G.M.; Eze, I.C.; Kress, S.; Wheelock, C.E.; Peters, A.; et al. Air Pollution, Metabolites and Respiratory Health across the Life-Course. Eur. Respir. Rev. 2022, 31, 220038. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Hansell, A.L.; Granell, R.; Blangiardo, M.; Zottoli, M.; Fecht, D.; Gulliver, J.; John Henderson, A.; Elliott, P. Prenatal, Early-Life, and Childhood Exposure to Air Pollution and Lung Function: The Alspac Cohort. Am. J. Respir. Crit. Care Med. 2020, 202, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.M.; Hoffmann, A.R.; Behlen, J.C.; Lau, C.; Pendleton, D.; Harvey, N.; Shore, R.; Li, Y.; Chen, J.; Tian, Y.; et al. Air Pollution and Children’s Health—A Review of Adverse Effects Associated with Prenatal Exposure from Fine to Ultrafine Particulate Matter. Environ. Health Prev. Med. 2021, 26, 72. [Google Scholar] [CrossRef] [PubMed]
- Hansell, A.; Cai, Y.; Granell, R.; Blangiardo, M.; Fecht, D.; Gulliver, J.; Henderson, J.; Elliott, P. Prenatal, Early-Life and Childhood Exposure to Air Pollution and Lung Function in the UK Avon Longitudinal Study of Parents and Children (ALSPAC) Cohort. Eur. Respir. J. 2019, 54, OA482. [Google Scholar] [CrossRef]
- Mirkasymov, A.B.; Zelepukin, I.V.; Ivanov, I.N.; Belyaev, I.B.; Dzhalilova, D.S.; Trushina, D.B.; Yaremenko, A.V.; Ivanov, V.Y.; Nikitin, M.P.; Nikitin, P.I.; et al. Macrophage Blockade Using Nature-Inspired Ferrihydrite for Enhanced Nanoparticle Delivery to Tumor. Int. J. Pharm. 2022, 621, 121795. [Google Scholar] [CrossRef] [PubMed]
- Yaremenko, A.V.; Zelepukin, I.V.; Ivanov, I.N.; Melikov, R.O.; Pechnikova, N.A.; Dzhalilova, D.S.; Mirkasymov, A.B.; Bragina, V.A.; Nikitin, M.P.; Deyev, S.M.; et al. Influence of Magnetic Nanoparticle Biotransformation on Contrasting Efficiency and Iron Metabolism. J. Nanobiotechnol. 2022, 20, 535. [Google Scholar] [CrossRef] [PubMed]
- Hancox, R.J.; Poulton, R.; Greene, J.M.; McLachlan, C.R.; Pearce, M.S.; Sears, M.R. Associations between Birth Weight, Early Childhood Weight Gain and Adult Lung Function. Thorax 2009, 64, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Svanes, Ø.; Skorge, T.D.; Johannessen, A.; Bertelsen, R.J.; Bràtveit, M.; Forsberg, B.; Gislason, T.; Holm, M.; Janson, C.; Jögi, R.; et al. Respiratory Health in Cleaners in Northern Europe: Is Susceptibility Established in Early Life? PLoS ONE 2015, 10, e0131959. [Google Scholar] [CrossRef] [PubMed]
- Domvri, K.; Yaremenko, A.V.; Apostolopoulos, A.; Petanidis, S.; Karachrysafi, S.; Pastelli, N.; Papamitsou, T.; Papaemmanouil, S.; Lampaki, S.; Porpodis, K. Expression Patterns and Clinical Implications of PDL1 and DLL3 Biomarkers in Small Cell Lung Cancer Retrospectively Studied: Insights for Therapeutic Strategies and Survival Prediction. Heliyon 2024, 10, e27208. [Google Scholar] [CrossRef] [PubMed]
- York, T.P.; Eaves, L.J.; Neale, M.C.; Strauss, J.F. The Contribution of Genetic and Environmental Factors to the Duration of Pregnancy. Am. J. Obstet. Gynecol. 2014, 210, 398. [Google Scholar] [CrossRef]
- Gyamfi-Bannerman, C.; Gilbert, S.; Landon, M.B.; Spong, C.Y.; Rouse, D.J.; Varner, M.W.; Meis, P.J.; Wapner, R.J.; Sorokin, Y.; Carpenter, M.; et al. Effect of Antenatal Corticosteroids on Respiratory Morbidity in Singletons after Late-Preterm Birth. Obstet. Gynecol. 2012, 119, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Tapia, J.L.; Urzua, S.; Bancalari, A.; Meritano, J.; Torres, G.; Fabres, J.; Toro, C.A.; Rivera, F.; Cespedes, E.; Burgos, J.F.; et al. Randomized Trial of Early Bubble Continuous Positive Airway Pressure for Very Low Birth Weight Infants. J. Pediatr. 2012, 161, 75–80.e1. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.T.; Baiden, F.; Brooks, J.C.; Morris, M.C.; Giessler, K.; Punguyire, D.; Apio, G.; Agyeman-Ampromfi, A.; Lopez-Pintado, S.; Sylverken, J.; et al. Continuous Positive Airway Pressure for Children with Undifferentiated Respiratory Distress in Ghana: An Open-Label, Cluster, Crossover Trial. Lancet Glob. Health 2017, 5, e615–e623. [Google Scholar] [CrossRef]
- Luzak, A.; Fuertes, E.; Flexeder, C.; Standl, M.; von Berg, A.; Berdel, D.; Koletzko, S.; Heinrich, J.; Nowak, D.; Schulz, H. Which Early Life Events or Current Environmental and Lifestyle Factors Influence Lung Function in Adolescents?—Results from the GINIplus & LISAplus Studies. Respir. Res. 2017, 18, 138. [Google Scholar] [CrossRef] [PubMed]
- Melén, E.; Guerra, S. Recent Advances in Understanding Lung Function Development. F1000Res 2017, 6, 726. [Google Scholar] [CrossRef] [PubMed]
- Carlo, W.A.; McDonald, S.A.; Fanaroff, A.A.; Vohr, B.R.; Stoll, B.J.; Ehrenkranz, R.A.; Andrews, W.W.; Wallace, D.; Das, A.; Bell, E.F.; et al. Association of Antenatal Corticosteroids with Mortality and Neurodevelopmental Outcomes among Infants Born at 22 to 25 Weeks’ Gestation. JAMA 2011, 306, 2348–2358. [Google Scholar] [CrossRef]
- Mori, R.; Kusuda, S.; Fujimura, M. Antenatal Corticosteroids Promote Survival of Extremely Preterm Infants Born at 22 to 23 Weeks of Gestation. J. Pediatr. 2011, 159, 110–114.e1. [Google Scholar] [CrossRef]
- Fujiwara, T.; Chida, S.; Watabe, Y.; Maeta, H.; Morita, T.; Abe, T. Artificial Surfactant Therapy in Hyaline-Membrane Disease. Lancet 1980, 1, 55–59. [Google Scholar] [CrossRef]
- Kalenga, M.; Gaultier, C.; Burri, P.H. Nutritional Aspects of Lung Development. In Lung Development; Springer: New York, NY, USA, 1999; pp. 347–363. [Google Scholar] [CrossRef]
- Bhatia, J.; Parish, A. Nutrition and the Lung. Neonatology 2009, 95, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Schlosser-Brandenburg, J.; Ebner, F.; Klopfleisch, R.; Kühl, A.A.; Zentek, J.; Pieper, R.; Hartmann, S. Influence of Nutrition and Maternal Bonding on Postnatal Lung Development in the Newborn Pig. Front. Immunol. 2021, 12, 734153. [Google Scholar] [CrossRef] [PubMed]
- Fandiño, J.; Toba, L.; González-Matías, L.C.; Diz-Chaves, Y.; Mallo, F. Perinatal Undernutrition, Metabolic Hormones, and Lung Development. Nutrients 2019, 11, 2870. [Google Scholar] [CrossRef] [PubMed]
- Merritt, T.A. Improving Fetal Lung Development with Vitamin C and Reducing Asthma in Children. J. Perinatol. 2018, 38, 775–777. [Google Scholar] [CrossRef] [PubMed]
- Becher, T.H.; Miedema, M.; Kallio, M.; Papadouri, T.; Karaoli, C.; Sophocleous, L.; Rahtu, M.; van Leuteren, R.W.; Waldmann, A.D.; Strodthoff, C.; et al. Prolonged Continuous Monitoring of Regional Lung Function in Infants with Respiratory Failure. Ann. Am. Thorac. Soc. 2022, 19, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Gallacher, D.J.; Hart, K.; Kotecha, S. Common Respiratory Conditions of the Newborn. Breathe 2016, 12, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.; Melbye, M.; Olsen, S.F.; Sørensen, T.I.A.; Aaby, P.; Nybo Andersen, A.M.; Taxbøl, D.; Hansen, K.D.; Juhl, M.; Schow, T.B.; et al. The Danish National Birth Cohort—Its Background, Structure and Aim. Scand. J. Public Health 2001, 29, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsdóttir, H.K.; Carlsen, O.C.L.; Bains, K.E.S.; Färdig, M.; Haugen, G.; Jonassen, C.M.; Leblanc, M.; Nordlund, B.; Rehbinder, E.M.; Skjerven, H.O.; et al. Infant Lung Function and Maternal Physical Activity in the First Half of Pregnancy. ERJ Open Res. 2022, 8, 00172-2022. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, A.R.; Gowler, H.; Curtis, F.; Holden, N.S.; Bridle, C.; Jones, A.W. Efficacy of Supervised Maintenance Exercise Following Pulmonary Rehabilitation on Health Care Use: A Systematic Review and Meta-Analysis. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 257. [Google Scholar] [CrossRef] [PubMed]
- Román, M.; Larraz, C.; Gómez, A.; Ripoll, J.; Mir, I.; Miranda, E.Z.; MacHo, A.; Thomas, V.; Esteva, M. Efficacy of Pulmonary Rehabilitation in Patients with Moderate Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. BMC Fam. Pract. 2013, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Rochester, C.L.; Alison, J.A.; Carlin, B.; Jenkins, A.R.; Cox, N.S.; Bauldoff, G.; Bhatt, S.P.; Bourbeau, J.; Burtin, C.; Camp, P.G.; et al. Pulmonary Rehabilitation for Adults with Chronic Respiratory Disease: An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2023, 208, e7–e26. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.; Ramirez, M.I.; Gern, J.E.; Cutting, G.; Redding, G.; Hagood, J.S.; Whitsett, J.; Abman, S.; Raj, J.U.; Barst, R.; et al. Strategic Plan for Pediatric Respiratory Diseases Research: An NHLBI Working Group Report. Proc. Am. Thorac. Soc. 2009, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.; Maricoto, T.; Costa, P.; Berger-Estilita, J.; Padilha, J.M. A Meta-Analysis on the Structure of Pulmonary Rehabilitation Maintenance Programmes on COPD Patients’ Functional Capacity. NPJ Prim. Care Respir. Med. 2022, 32, 38. [Google Scholar] [CrossRef]
- Elsaeed Saad Elmorshidy, B.; Gamal Amer Elkholy, M.; Mohamed Elsaadany, H.; Mohamed Mansour, Y.; Samir Sharshar, R.; Mokhtar Bahr, H. Effect of Pulmonary Rehabilitation Programme Including Either O2 Inhalation or Noninvasive Ventilation in Patients with Chronic Obstructive Pulmonary Disease. Can. J. Respir. Ther. 2023, 59, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Franssen, F.M.E.; Alter, P.; Bar, N.; Benedikter, B.J.; Iurato, S.; Maier, D.; Maxheim, M.; Roessler, F.K.; Spruit, M.A.; Vogelmeier, C.F.; et al. Personalized Medicine for Patients with COPD: Where Are We? Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1465. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, S.; McCarthy, V.J.C.; Queally, M.; Savage, E. The Preferences of People with Asthma or Chronic Obstructive Pulmonary Disease for Self-Management Support: A Qualitative Descriptive Study. J. Clin. Nurs. 2021, 30, 2832–2841. [Google Scholar] [CrossRef]
- van de Hei, S.J.; Dierick, B.J.H.; Aarts, J.E.P.; Kocks, J.W.H.; van Boven, J.F.M. Personalized Medication Adherence Management in Asthma and Chronic Obstructive Pulmonary Disease: A Review of Effective Interventions and Development of a Practical Adherence Toolkit. J. Allergy Clin. Immunol. Pract. 2021, 9, 3979–3994. [Google Scholar] [CrossRef] [PubMed]
- Cravo, A.; Attar, D.; Freeman, D.; Holmes, S.; Ip, L.; Singh, S.J. The Importance of Self-Management in the Context of Personalized Care in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2022, 17, 231. [Google Scholar] [CrossRef] [PubMed]
- Fuertes, E.; Markevych, I.; Thomas, R.; Boyd, A.; Granell, R.; Mahmoud, O.; Heinrich, J.; Garcia-Aymerich, J.; Roda, C.; Henderson, J.; et al. Residential Greenspace and Lung Function up to 24 Years of Age: The ALSPAC Birth Cohort. Environ. Int. 2020, 140, 105749. [Google Scholar] [CrossRef] [PubMed]
- Gregory, D.J.; Kobzik, L.; Yang, Z.; McGuire, C.C.; Fedulov, A.V. Transgenerational Transmission of Asthma Risk after Exposure to Environmental Particles during Pregnancy. Am. J. Physiol. Lung Cell. Mol. Physiol. 2017, 313, L395–L405. [Google Scholar] [CrossRef] [PubMed]
- Cárdenes, N.; Sembrat, J.; Noda, K.; Lovelace, T.; Álvarez, D.; Bittar, H.E.T.; Philips, B.J.; Nouraie, M.; Benos, P.V.; Sánchez, P.G.; et al. Human Ex Vivo Lung Perfusion: A Novel Model to Study Human Lung Diseases. Sci. Rep. 2021, 11, 490. [Google Scholar] [CrossRef] [PubMed]
- Sucre, J.M.S.; Vickers, K.C.; Benjamin, J.T.; Plosa, E.J.; Jetter, C.S.; Cutrone, A.; Ransom, M.; Anderson, Z.; Sheng, Q.; Fensterheim, B.A.; et al. Hyperoxia Injury in the Developing Lung Is Mediated by Mesenchymal Expression of Wnt5A. Am. J. Respir. Crit. Care Med. 2020, 201, 1249–1262. [Google Scholar] [CrossRef] [PubMed]
- Aros, C.J.; Pantoja, C.J.; Gomperts, B.N. Wnt Signaling in Lung Development, Regeneration, and Disease Progression. Commun. Biol. 2021, 4, 601. [Google Scholar] [CrossRef] [PubMed]
- Storti, M.; Faietti, M.L.; Murgia, X.; Catozzi, C.; Minato, I.; Tatoni, D.; Cantarella, S.; Ravanetti, F.; Ragionieri, L.; Ciccimarra, R.; et al. Time-Resolved Transcriptomic Profiling of the Developing Rabbit’s Lungs: Impact of Premature Birth and Implications for Modelling Bronchopulmonary Dysplasia. Respir. Res. 2023, 24, 80. [Google Scholar] [CrossRef] [PubMed]
- Abman, S.H.; Sun, X. Mechanistic Insights into Lethal Lung Developmental Disorders. Am. J. Respir. Crit. Care Med. 2019, 200, 1087–1089. [Google Scholar] [CrossRef] [PubMed]
- Mørkve Knudsen, T.; Rezwan, F.I.; Jiang, Y.; Karmaus, W.; Svanes, C.; Holloway, J.W. Transgenerational and Intergenerational Epigenetic Inheritance in Allergic Diseases. J. Allergy Clin. Immunol. 2018, 142, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Pembrey, M.; Saffery, R.; Bygren, L.O. Human Transgenerational Responses to Early-Life Experience: Potential Impact on Development, Health and Biomedical Research. J. Med. Genet. 2014, 51, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Onland, W.; Hutten, J.; Miedema, M.; Bos, L.D.; Brinkman, P.; Maitland-van der Zee, A.H.; van Kaam, A.H. Precision Medicine in Neonates: Future Perspectives for the Lung. Front. Pediatr. 2020, 8, 586061. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Han, D.; Wang, X.; Huang, X.; Huang, Z.; Liu, Y.; Zhong, J.; Walther, F.J.; Yang, C.; Wagenaar, G.T.M. Vascular and Pulmonary Effects of Ibuprofen on Neonatal Lung Development. Respir. Res. 2023, 24, 39. [Google Scholar] [CrossRef] [PubMed]
- Barrette, A.M.; Roberts, J.K.; Chapin, C.; Egan, E.A.; Segal, M.R.; Oses-Prieto, J.A.; Chand, S.; Burlingame, A.L.; Ballard, P.L. Antiinflammatory Effects of Budesonide in Human Fetal Lung. Am. J. Respir. Cell Mol. Biol. 2016, 55, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Plichta, J.; Kuna, P.; Panek, M. Biologic Drugs in the Treatment of Chronic Inflammatory Pulmonary Diseases: Recent Developments and Future Perspectives. Front Immunol 2023, 14, 1207641. [Google Scholar] [CrossRef] [PubMed]
- Adamič, N.; Vengust, M. Regenerative Medicine in Lung Diseases: A Systematic Review. Front. Vet. Sci. 2023, 10, 1115708. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Thébaud, B. Stem Cell Biology and Regenerative Medicine for Neonatal Lung Diseases. Pediatr. Res. 2017, 83, 291–297. [Google Scholar] [CrossRef]
- Khalaj, K.; Figueira, R.L.; Antounians, L.; Gandhi, S.; Wales, M.; Montalva, L.; Biouss, G.; Zani, A. Treatment with Amniotic Fluid Stem Cell Extracellular Vesicles Promotes Fetal Lung Branching and Cell Differentiation at Canalicular and Saccular Stages in Experimental Pulmonary Hypoplasia Secondary to Congenital Diaphragmatic Hernia. Stem Cells Transl. Med. 2022, 11, 1089–1102. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Valizadeh, H.; Alipourfard, I.; Bidares, R.; Aghebati-Maleki, L.; Ahmadi, M. Epigenetic Modifications and Therapy in Chronic Obstructive Pulmonary Disease (COPD): An Update Review. COPD 2020, 17, 333–342. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yaremenko, A.V.; Pechnikova, N.A.; Porpodis, K.; Damdoumis, S.; Aggeli, A.; Theodora, P.; Domvri, K. Association of Fetal Lung Development Disorders with Adult Diseases: A Comprehensive Review. J. Pers. Med. 2024, 14, 368. https://doi.org/10.3390/jpm14040368
Yaremenko AV, Pechnikova NA, Porpodis K, Damdoumis S, Aggeli A, Theodora P, Domvri K. Association of Fetal Lung Development Disorders with Adult Diseases: A Comprehensive Review. Journal of Personalized Medicine. 2024; 14(4):368. https://doi.org/10.3390/jpm14040368
Chicago/Turabian StyleYaremenko, Alexey V., Nadezhda A. Pechnikova, Konstantinos Porpodis, Savvas Damdoumis, Amalia Aggeli, Papamitsou Theodora, and Kalliopi Domvri. 2024. "Association of Fetal Lung Development Disorders with Adult Diseases: A Comprehensive Review" Journal of Personalized Medicine 14, no. 4: 368. https://doi.org/10.3390/jpm14040368