
Iatrogenic Cerebrospinal Fluid Leak in Endoscopic Sinus Surgery: Topographical Map and Influence of Skull Base Asymmetry

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Management and Study Variables
2.2. Study Objectives
2.3. Statistical Analysis
3. Results
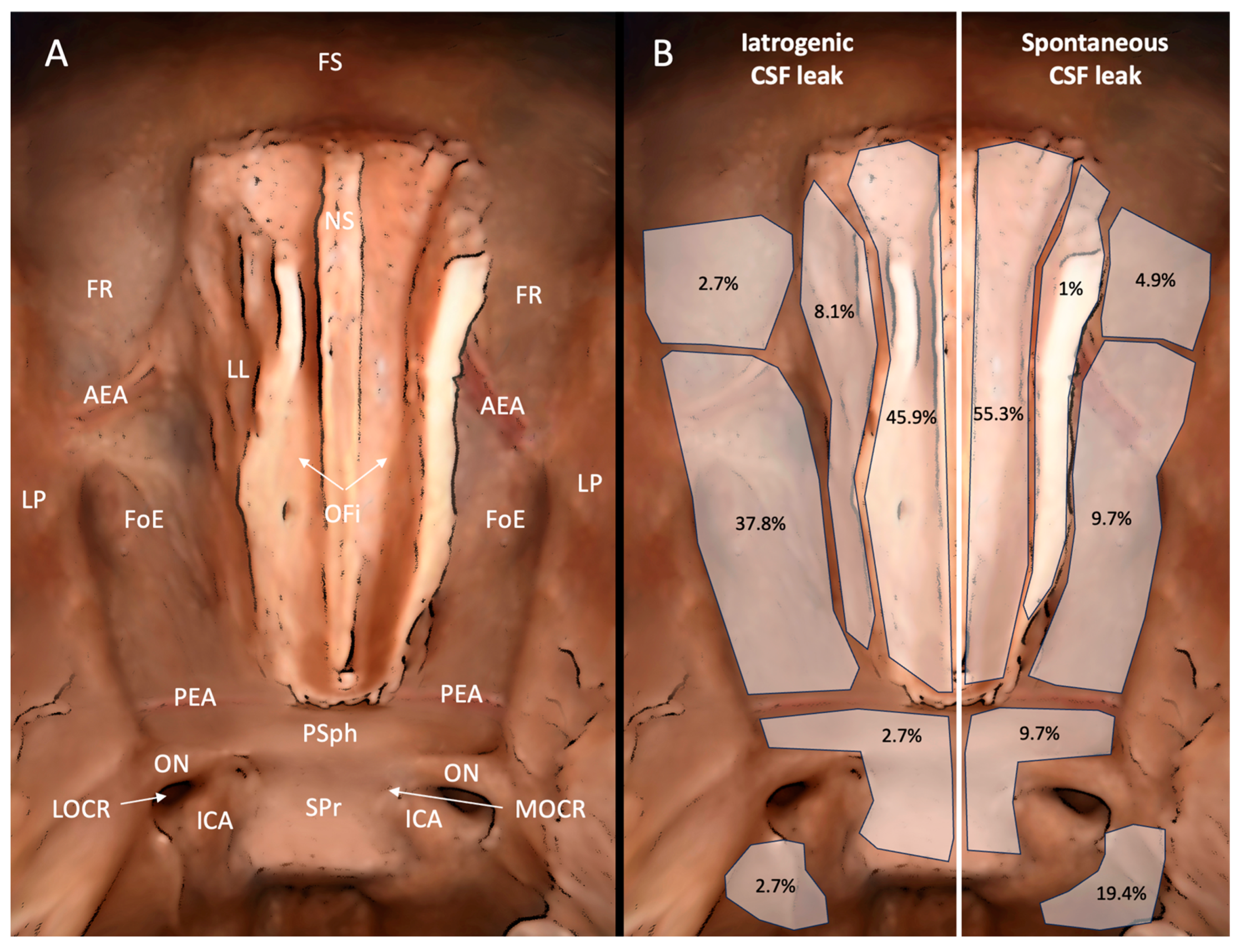
3.1. Analysis of Topographic Features
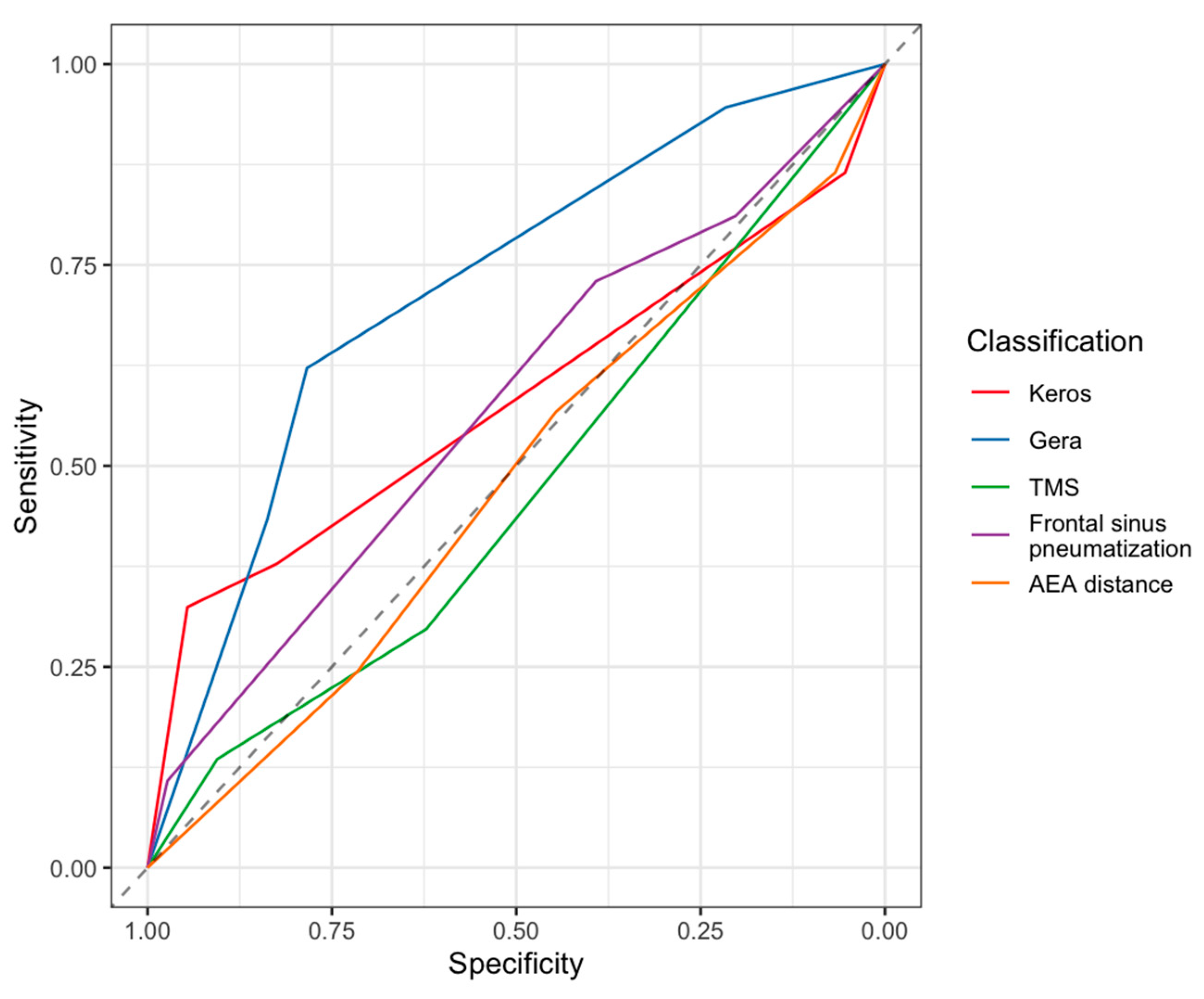
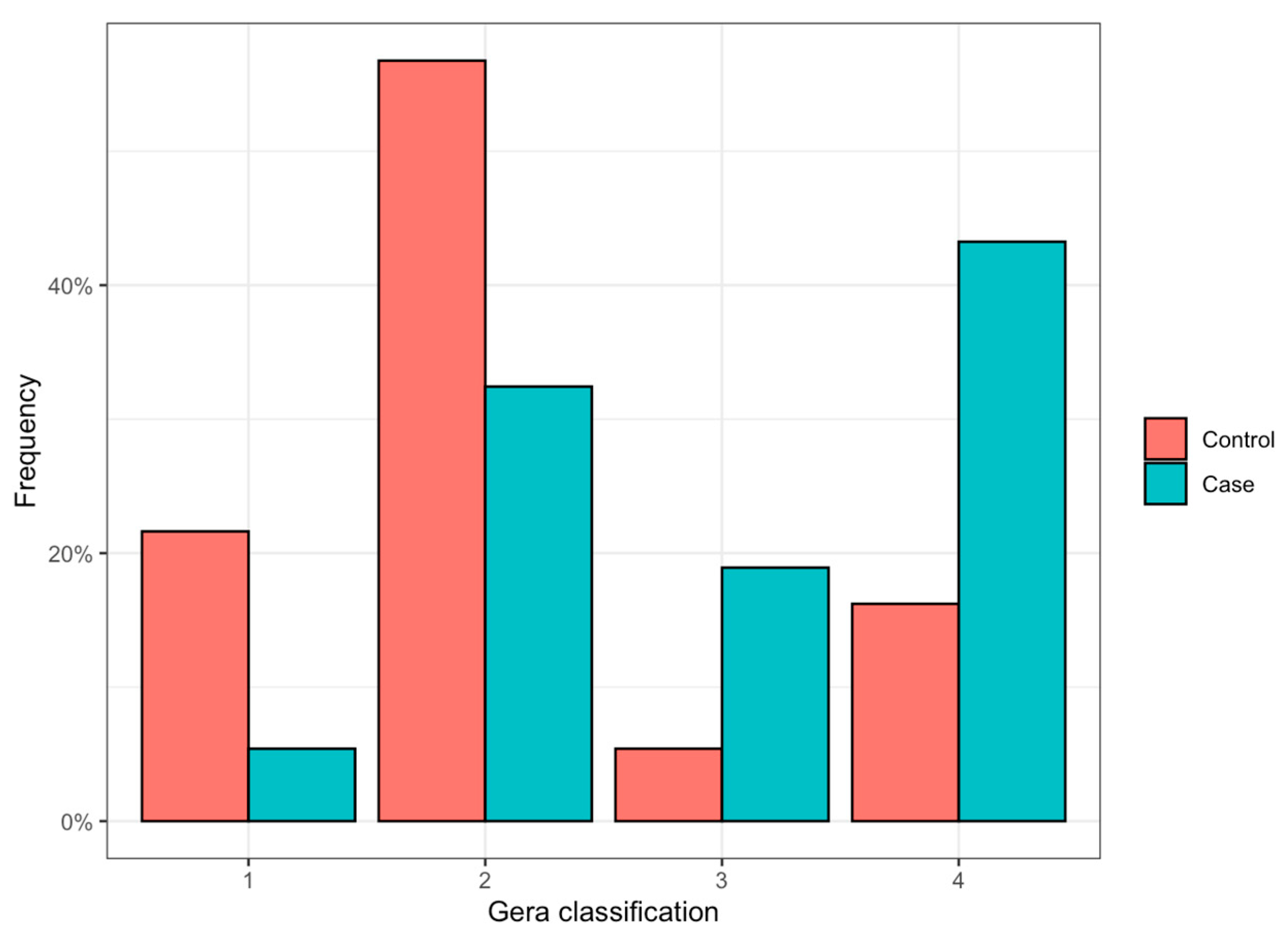
3.2. Iatrogenic CSF Leak and Skull Base Anatomy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kerr, J.T.; Chu, F.W.K.; Bayles, S.W. Cerebrospinal fluid rhinorrhea: Diagnosis and management. Otolaryngol. Clin. N. Am. 2005, 38, 597–611. [Google Scholar] [CrossRef]
- Bedrosian, J.C.; Anand, V.K.; Schwartz, T.H. The endoscopic endonasal approach to repair of iatrogenic and noniatrogenic cerebrospinal fluid leaks and encephaloceles of the anterior cranial fossa. World Neurosurg. 2014, 82, S86–S94. [Google Scholar] [CrossRef]
- Ledderose, G.J.; Stelter, K.; Betz, C.S.; Englhard, A.S.; Ledderose, C.; Leunig, A. Cerebrospinal fluid leaks during endoscopic sinus surgery in thirty-two patients. Clin. Otolaryngol. 2017, 42, 1105–1108. [Google Scholar] [CrossRef]
- Kubik, M.; Lee, S.; Snyderman, C.; Wang, E. Neurologic sequelae associated with delayed identification of iatrogenic skull base injury during endoscopic sinus surgery (ESS). Rhinology 2017, 55, 53–58. [Google Scholar] [CrossRef]
- Gera, R.; Mozzanica, F.; Karligkiotis, A.; Preti, A.; Bandi, F.; Gallo, S.; Schindler, A.; Bulgheroni, C.; Ottaviani, F.; Castelnuovo, P. Lateral lamella of the cribriform plate, a keystone landmark: Proposal for a novel classification system. Rhinology 2018, 56, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Dessi, P.; Castro, F.; Triglia, J.M.; Zanaret, M.; Cannoni, M. Major complications of sinus surgery: A review of 1192 procedures. J. Laryngol. Otol. 1994, 108, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Keros, P. On the practical value of differences in the level of the lamina cribrosa of the ethmoid. Z. Laryngol. Rhinol. Otol. 1962, 41, 809–813. [Google Scholar] [PubMed]
- Yazici, D. The effect of frontal sinus pneumatization on anatomic variants of paranasal sinuses. Eur. Arch. Otorhinolaryngol. 2019, 276, 1049–1056. [Google Scholar] [CrossRef]
- Abdullah, B.; Lim, E.H.; Husain, S.; Snidvongs, K.; Wang, D.Y. Anatomical variations of anterior ethmoidal artery and their significance in endoscopic sinus surgery: A systematic review. Surg. Radiol. Anat. 2019, 41, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, B.; Chew, S.C.; Aziz, M.E.; Shukri, N.M.; Husain, S.; Joshua, S.W.; Wang, D.Y.; Snidvongs, K. A new radiological classification for the risk assessment of anterior skull base injury in endoscopic sinus surgery. Sci. Rep. 2020, 10, 4600. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.; Mao, S.; Li, D.; Ye, H.; Zhang, W. Treatment and Outcomes of Iatrogenic Cerebrospinal Fluid Leak Caused by Different Surgical Procedures. World Neurosurg. 2020, 143, e667–e675. [Google Scholar] [CrossRef] [PubMed]
- Adeel, M.; Ikram, M.; Rajput, M.S.A.; Arain, A.; Khattak, Y.J. Asymmetry of lateral lamella of the cribriform plate: A software-based analysis of coronal computed tomography and its clinical relevance in endoscopic sinus surgery. Surg. Radiol. Anat. 2013, 35, 843–847. [Google Scholar] [CrossRef]
- Molodianovitch, K.; Faraggi, D.; Reiser, B. Comparing the areas under two correlated ROC curves: Parametric and non-parametric approaches. Biom. J. 2006, 48, 745–757. [Google Scholar] [CrossRef] [PubMed]
- Preti, A.; Mozzanica, F.; Gera, R.; Gallo, S.; Zocchi, J.; Bandi, F.; Guidugli, G.; Ambrogi, F.; Yakirevitch, A.; Schindler, A.; et al. Horizontal lateral lamella as a risk factor for iatrogenic cerebrospinal fluid leak. Clinical retrospective evaluation of 24 cases. Rhinology 2018, 56, 358–363. [Google Scholar] [CrossRef]
- Algin, O.; Hakyemez, B.; Gokalp, G.; Ozcan, T.; Korfali, E.; Parlak, M. The contribution of 3D-CISS and contrast-enhanced MR cisternography in detecting cerebrospinal fluid leak in patients with rhinorrhoea. Br. J. Radiol. 2010, 83, 225–232. [Google Scholar] [CrossRef]
- Georgalas, C.; Oostra, A.; Ahmed, S.; Castelnuovo, P.; Dallan, I.; van Furth, W.; Harvey, R.J.; Herman, P.; Kombogiorgas, D.; Locatelli, D.; et al. International Consensus Statement: Spontaneous Cerebrospinal Fluid Rhinorrhea. Int. Forum Allergy Rhinol. 2021, 11, 794–803. [Google Scholar] [CrossRef]
- Jankowski, R.; Bodino, C. Evolution of symptoms associated to nasal polyposis following oral steroid treatment and nasalization of the ethmoid–radical ethmoidectomy is functional surgery for NPS. Rhinology 2003, 41, 211–219. [Google Scholar]
- Barañano, C.F.; Curé, J.; Palmer, J.N.; Woodworth, B.A. Sternberg’s canal: Fact or fiction? Am. J. Rhinol. Allergy 2009, 23, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Song, Y.J.; Chung, Y.S.; Lee, B.J.; Yong, J.J. Height and shape of the skull base as risk factors for skull base penetration during endoscopic sinus surgery. Ann. Otol. Rhinol. Laryngol. 2007, 116, 199–205. [Google Scholar] [CrossRef]
- Skorek, A.; Tretiakow, D.; Szmuda, T.; Przewozny, T. Is the Keros classification alone enough to identify patients with the “dangerous ethmoid”? An anatomical study. Acta Otolaryngol. 2017, 137, 196–201. [Google Scholar] [CrossRef]
- Fadda, G.L.; Petrelli, A.; Martino, F.; Succo, G.; Castelnuovo, P.; Bignami, M.; Cavallo, G. Anatomic Variations of Ethmoid Roof and Risk of Skull Base Injury in Endoscopic Sinus Surgery: Statistical Correlations. Am. J. Rhinol. Allergy 2021, 35, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Pawar, A.; Konde, S.; Bhole, P. Assessment of depth of olfactory fossa in pre-functional endoscopic sinus surgery computed tomography scan of paranasal sinuses. Int. J. Otorhinolaryngol. Head. Neck Surg. 2018, 4, 83–86. [Google Scholar] [CrossRef]
- Lebowitz, R.A.; Terk, A.; Jacobs, J.B.; Holliday, R.A. Asymmetry of the ethmoid roof: Analysis using coronal computed tomography. Laryngoscope 2001, 111, 2122–2124. [Google Scholar] [CrossRef] [PubMed]
- Alazzawi, S.; Omar, R.; Rahmat, K.; Alli, K. Radiological analysis of the ethmoid roof in the Malaysian population. Auris Nasus Larynx 2012, 39, 393–396. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Iatrogenic CSF Leak | Spontaneous CSF Leak | Traumatic CSF Leak | |
|---|---|---|---|
| No. patients | 37 | 103 | 13 |
| Age at surgery. Mean (SD) | 47.5 (15.2) | 51.9 (15.1) | 50.9 (15.2) |
| Sex, male/female | 24:13 | 31:72 | 10:3 |
| Side, right/left | 17:20 | 47:56 | 7:6 |
| Radiological sign of intracranial hypertension, N (%) | 2 (5.4%) | 60 (58.3%) | 3 (23.1%) |
| Post-operative antibiotics, N (%) | 2 (5.4%) | 3 (2.9%) | 1 (7.7%) |
| Post-operative complications, N (%) | 1 (2.7%) | 2 (1.9%) | 3 (23.1%) |
| Recurrence, N (%) | 1 (2.7%) | 4 (3.9%) | 1 (7.7%) |
| Iatrogenic CSF Leak | Spontaneous CSF Leak | Traumatic CSF Leak | |
|---|---|---|---|
| Posterior plate of the frontal sinus/frontal recess | 1 (2.7%) | 5 (4.9%) | 2 (15.4%) |
| Fovea ethmoidalis | 14 (37.8%) | 10 (9.7%) | 4 (30.8%) |
| Lateral lamella | 3 (8.1%) | 1 (1%) | 1 (7.7%) |
| Cribriform plate | 17 (45.9%) | 57 (55.3%) | 1 (7.7%) |
| Planum sphenoidalis and posterior wall of the sphenoidal sinus | 1 (2.7%) | 10 (9.7%) | 3 (23.1%) |
| Lateral wall of the sphenoidal sinus | 1 (2.7%) | 20 (19.4%) | 2 (15.4%) |
| Iatrogenic CSF Leak Group N = 37 | Control Group N = 74 | AUC (95% CI) | |
|---|---|---|---|
| Gera classification | |||
| Class I (>80°, low risk) | 2 (5.4%) | 16 (21.6%) | 0.719 (0.624–0.813) |
| Class II (45–80°, medium risk) | 12 (32.4%) | 42 (56.8%) | |
| Class III (<45°, high risk) | 7 (18.9%) | 4 (5.4%) | |
| Class IV (asymmetry > 15°) | 16 (43.3%) | 12 (16.2%) | |
| Keros classification | |||
| Type I (1–3 mm) | 5 (13.5%) | 4 (5.4%) | 0.581 (0.469–0.692) |
| Type II (4–7 mm) | 18 (48.7%) | 57 (77%) | |
| Type III (8–16 mm) | 2 (5.4%) | 9 (12.2%) | |
| Type IV (asymmetry) | 12 (32.4%) | 4 (5.4%) | |
| Frontal sinus pneumatization | |||
| Aplasia–hypoplasia | 4 (10.8%) | 2 (2.7%) | 0.574 (0.471–0.677) |
| Pneumatization medial to the midorbital line | 23 (62.2%) | 43 (58.1%) | |
| Hyperplasia | 3 (8.1%) | 14 (18.9%) | |
| Asymmetry | 7 (18.9%) | 15 (20.3%) | |
| AEA distance from the SB | |||
| AEA included in the SB | 9 (24.4%) | 21 (28.4%) | 0.478 (0.367–0.589) |
| AEA under the SB | 12 (32.4%) | 20 (27%) | |
| AEA runs freely at a distance below the SB | 11 (29.8%) | 28 (37.8%) | |
| Asymmetry | 5 (13.4%) | 5 (6.8%) | |
| Thailand–Malaysia–Singapore score (TMS) | |||
| Type 1 (OF-CP and OF-ER >10 mm) | 26 (70.3%) | 46 (62.1%) | 0.471 (0.373–0.569) |
| Type 2 (OF-CP or OF-ER < 10 mm) | 6 (16.3%) | 21 (28.4%) | |
| Type 3 (OF-CP and OF-ER < 10 mm) | 0 (0%) | 0 (0%) | |
| Type 4 (asymmetry) | 5 (13.4%) | 7 (9.5%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinciguerra, A.; Dohin, I.; Daloiso, A.; Boaria, F.; Marc, M.; Verillaud, B.; Chatelet, F.; Herman, P. Iatrogenic Cerebrospinal Fluid Leak in Endoscopic Sinus Surgery: Topographical Map and Influence of Skull Base Asymmetry. J. Pers. Med. 2024, 14, 226. https://doi.org/10.3390/jpm14030226
Vinciguerra A, Dohin I, Daloiso A, Boaria F, Marc M, Verillaud B, Chatelet F, Herman P. Iatrogenic Cerebrospinal Fluid Leak in Endoscopic Sinus Surgery: Topographical Map and Influence of Skull Base Asymmetry. Journal of Personalized Medicine. 2024; 14(3):226. https://doi.org/10.3390/jpm14030226
Chicago/Turabian StyleVinciguerra, Alessandro, Isabelle Dohin, Antonio Daloiso, Francesco Boaria, Morgane Marc, Benjamin Verillaud, Florian Chatelet, and Philippe Herman. 2024. "Iatrogenic Cerebrospinal Fluid Leak in Endoscopic Sinus Surgery: Topographical Map and Influence of Skull Base Asymmetry" Journal of Personalized Medicine 14, no. 3: 226. https://doi.org/10.3390/jpm14030226