

Rare Solid Pancreatic Lesions on Cross-Sectional Imaging
by
 , ,
, ,
Ana Veron Sanchez
1,*,
Nuria Santamaria Guinea
2,
Silvia Cayon Somacarrera
3,
Ilias Bennouna
1,
Martina Pezzullo
4 and
Maria Antonietta Bali
1 1
Hôpital Universitaire de Bruxelles, Institut Jules Bordet, 1070 Brussels, Belgium
2
Clatterbridge Cancer Centre, Liverpool L7 8YA, UK
3
Hospital Universitario Marques de Valdecilla, 39008 Santander, Spain
4
Hôpital Universitaire de Bruxelles, Hôpital Erasme, 1070 Brussels, Belgium
*
Author to whom correspondence should be addressed.
Diagnostics 2023, 13(16), 2719; https://doi.org/10.3390/diagnostics13162719
Submission received: 31 July 2023
/
Revised: 15 August 2023
/
Accepted: 18 August 2023
/
Published: 21 August 2023
(This article belongs to the Special Issue Imaging Diagnosis in Abdomen)
Abstract
:Several solid lesions can be found within the pancreas mainly arising from the exocrine and endocrine pancreatic tissue. Among all pancreatic malignancies, the most common subtype is pancreatic ductal adenocarcinoma (PDAC), to a point that pancreatic cancer and PDAC are used interchangeably. But, in addition to PDAC, and to the other most common and well-known solid lesions, either related to benign conditions, such as pancreatitis, or not so benign, such as pancreatic neuroendocrine neoplasms (pNENs), there are solid pancreatic lesions considered rare due to their low incidence. These lesions may originate from a cell line with a differentiation other than exocrine/endocrine, such as from the nerve sheath as for pancreatic schwannoma or from mesenchymal cells as for solitary fibrous tumour. These rare solid pancreatic lesions may show a behaviour that ranges in a benign to highly aggressive malignant spectrum. This review includes cases of an intrapancreatic accessory spleen, pancreatic tuberculosis, solid serous cystadenoma, solid pseudopapillary tumour, pancreatic schwannoma, purely intraductal neuroendocrine tumour, pancreatic fibrous solitary tumour, acinar cell carcinoma, undifferentiated carcinoma with osteoclastic-like giant cells, adenosquamous carcinoma, colloid carcinoma of the pancreas, primary leiomyosarcoma of the pancreas, primary and secondary pancreatic lymphoma and metastases within the pancreas. Therefore, it is important to determine the correct diagnosis to ensure optimal patient management. Because of their rarity, their existence is less well known and, when depicted, in most cases incidentally, the correct diagnosis remains challenging. However, there are some typical imaging features present on cross-sectional imaging modalities that, taken into account with the clinical and biological context, contribute substantially to achieve the correct diagnosis.
1. Introduction
In addition to the most common solid pancreatic lesions related to benign conditions, such as chronic pancreatitis, or to malignancy mainly represented by PDAC and pNENs, there are several rare pancreatic solid lesions that can be very challenging to correctly diagnose due to knowledge scarcity secondary to their very low incidence.
A variety of epithelial tumours may arise within the pancreas, with ductal, acinar and neuroendocrine differentiation. In addition, most of the mesenchymal tumours found in extrapancreatic locations may also arise within the pancreas. However, in cases such as the solid pseudopapillary neoplasm, there is no defined cell lineage identified.
These lesions can present a benign, potentially malignant and malignant behaviour and may show typical and atypical imaging features on cross-sectional imaging modalities. Combining these imaging findings with epidemiological, clinical and biological data may contribute to achieving the correct diagnosis.
Table 1 reports the rare solid pancreatic lesions classified in three sections based on their behaviour: benign, potentially malignant and malignant.
Due to their rarity, statistical data regarding the incidence and prevalence are not easy to find and published literature about these pancreatic lesions mainly consists of case reports or series. Table 2 reports incidence/prevalence data of these rare solid pancreatic lesions. Therefore, the aim of this pictorial review is to gather rare solid lesions that can be encountered in the pancreas and describe the cross-sectional imaging features, highlighting their respective hallmarks, with a focus on differential diagnosis and on patient management.
Concerning image acquisition, it is crucial to note the importance of including a pancreatic parenchymal phase, obtained 35–40 s after intravenous contrast administration, as it ensures a relatively increased enhancement of the pancreatic parenchyma and shows higher differences in attenuation between normal parenchyma and hypovascular tumours, as well as allowing assessment of arteries [1]. This parenchymal phase is followed by a portal venous phase, obtained at 70 s, to assess the veins, as venous flow artifacts observed in the pancreatic phase will be avoided [1]. In addition, hepatic enhancement will be increased and metastases will be detected more easily. Dynamic study finishes with a delayed venous phase, at 180 s.
2. Benign Lesions (Table S1)
2.1. Intrapancreatic Splenic Tissue (Figure 1)
Intrapancreatic splenic tissue (IPST) may occur under the form of accessory spleen or splenosis. Accessory spleens are congenital abnormalities, in which the earliest forms of spleen fail to fuse during the fifth week of embryonic life [2] and are usually located next to their embryonic origin or along their migration path [3]. Splenosis, though, is an acquired condition, in which a heterotopic transplantation of splenic tissue takes place [4], frequently after spleen surgery or trauma. It can be found anywhere throughout the abdomen, the pelvis and even the chest [5], although it occurs most frequently in the liver [6] and is rare within the pancreas [7]. Sixty-one accessory spleens were found within the pancreatic tail in a 3000-patient autopsy study [8].
The pancreatic tail is a preferred IPST location, either in the form of IPAS or splenosis [9] and it has been described as the second most common site of accessory spleen [10].
IPST commonly appears incidentally on cross-sectional techniques as a well-defined nodule, presenting clear demarcated borders with the adjacent parenchyma. It shows the same signal intensity as the spleen, with the same behaviour following intravenous contrast administration, heterogeneously enhancing in a zebra-pattern, during the arterial phase [11] due to different flow rate of contrast through the red and white pulp [12], and becoming homogeneous during the portal phase. However, this heterogeneous enhancement may be missing, especially in small lesions [11]. An elevated signal intensity in diffusion-weighted images (DWIs) using a high b-value is also suggestive of IPST [13]. IPST may grow and potentially mimic malignancy [14].
Spleen surgery or trauma history may be very helpful to achieve a correct diagnosis that is crucial to avoid unnecessary surgery or biopsy.
IPST should be included in the differential diagnosis of pancreatic hypervascular lesions, namely pNENs, solid pseudopapillary tumour (SPT) and pancreatic metastasis (PM) from renal clear cell carcinoma (RCC). Epidermoid cyst and inflammatory pseudotumour have been described as associated with IST [15,16,17], and the diagnosis under these circumstances may be challenging.
Tc-99m-labelled heat-denatured red blood cells (Tc-99m-DRBCs) are currently the gold standard technique to specifically prove the diagnosis of IST [18], as Tc-99m-DRBCs are trapped by reticuloendothelial cells.
Figure 1.
(A): axial T2-weighted images (T2WIs), (B): DWI, (C): axial T2WI-DWI fused images, (D): non-contrast-enhanced (NCE) fat-saturated (FS) T1-weighted images (T1WI), (E–G): axial contrast-enhanced (CE) dynamic FST1WI, (E): pancreatic parenchymal phase, (F): portal venous phase, (G): delayed venous phase, (H): Ga-68-DOTATOC PET-CT. Incidentally discovered IPAS in a 56 year-old patient, during check-up examination for elevation of pancreatic enzymes. Note a slightly hyperintense lesion within the pancreatic tail in T2WI (arrow in (A)), with diffusion restriction (arrow in (B,C)), conspicuous in the unenhanced phase (arrow in (D)) but not so much following intravenous contrast administration (arrow in (E–G)). Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) obtained small epithelioid cells, with antichromogranin- and synaptophysin-positive immunostaining and concluded a pNEN grade II (Ki 67 = 5%). However, in the PET-CT, the lesion (arrow in (H)) showed the same uptake as the spleen (* in (H)) and no non-physiological uptake was found, so an IPAS was suspected on imaging. The FNA result was a false positive for NEN secondary to contamination of normal neuroendocrine pancreatic tissue as the patient underwent a left-sided pancreatectomy with spleen preservation and the histological examination concluded IPAS.
Figure 1.
(A): axial T2-weighted images (T2WIs), (B): DWI, (C): axial T2WI-DWI fused images, (D): non-contrast-enhanced (NCE) fat-saturated (FS) T1-weighted images (T1WI), (E–G): axial contrast-enhanced (CE) dynamic FST1WI, (E): pancreatic parenchymal phase, (F): portal venous phase, (G): delayed venous phase, (H): Ga-68-DOTATOC PET-CT. Incidentally discovered IPAS in a 56 year-old patient, during check-up examination for elevation of pancreatic enzymes. Note a slightly hyperintense lesion within the pancreatic tail in T2WI (arrow in (A)), with diffusion restriction (arrow in (B,C)), conspicuous in the unenhanced phase (arrow in (D)) but not so much following intravenous contrast administration (arrow in (E–G)). Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) obtained small epithelioid cells, with antichromogranin- and synaptophysin-positive immunostaining and concluded a pNEN grade II (Ki 67 = 5%). However, in the PET-CT, the lesion (arrow in (H)) showed the same uptake as the spleen (* in (H)) and no non-physiological uptake was found, so an IPAS was suspected on imaging. The FNA result was a false positive for NEN secondary to contamination of normal neuroendocrine pancreatic tissue as the patient underwent a left-sided pancreatectomy with spleen preservation and the histological examination concluded IPAS.

2.2. Pancreatic Tuberculosis (Figure 2)
Pancreatic tuberculosis (PT) occurs very rarely, predominantly during a multiorgan abdominal spread of the infection [19]. Only 116 cases have been reported in the literature [20]. When isolated, its diagnosis is not suspected and is frequently achieved after histologic examination, following resection [21]. It has been theorised that pancreatic enzymes serve as shields against Mycobacterium tuberculosis [22].
In the western world, PT occurs mainly in immunocompromised patients [21,23]. It seems to be more frequent between the fourth and fifth decades of life [24,25]. Gender association is not clear [26,27].
The most frequent clinical presentations are vague non-specific symptoms (fatigue, fever, weight loss, nausea and vomiting) [28] or a history of acute or chronic pancreatitis [21]. Less frequently, it can also present as obstructive jaundice or gastrointestinal bleeding [29].
Presentation patterns are focal masses [31], multiple small nodules [23] and, less frequently, a diffuse involvement, mimicking an acute pancreatitis [32], with increased signal intensity in T2-weighted images (T2WIs) [21].
Focal pattern PT may appear as a well-defined cystic–solid mass, with varying aspects depending on the proportion of cystic and solid components [23]: hypodense on CT, hypo- or isointense in T1-weighted images (T1WIs) and heterogeneous in T2WIs. After intravenous contrast administration, peripheral enhancement with central necrosis or enhancing solid components may be depicted [25]. When predominantly cystic, PT may be misdiagnosed as a cystic tumour, such as a cystadenoma, a pseudocyst in the setting of chronic pancreatitis or an infected abscess. If, on the other hand, PT consists of a mainly solid lesion associated with biliary or main pancreatic duct (MPD) dilatation, it may be indistinguishable from PDAC (especially if accompanied by peripancreatic lymph nodes and signs of vascular invasion), lymphoma and metastasis [33].
Calcifications are frequently encountered [34]. Dilatation of the bile and pancreatic ducts may occur, though infrequently, despite the mass effect on the ducts [28]. Displacement and stenosis of an otherwise normal MPD are frequent features, without much prestenotic dilatation [34]. Vascular invasion has been described [25,35].
As lymph nodes are the most common tuberculosis site within the abdomen, accompanying peripancreatic lymphadenopathy is frequently found [36], mostly showing peripheral enhancement with central low attenuation, corresponding to granulation tissue encircling central caseous necrosis [37]. This appearance, although highly suggestive, is not pathognomonic of PT.
Both cytology and histological examination following imaging-guided fine-needle aspiration (FNA) or biopsy (FNB), respectively, are the gold standard diagnosing techniques. PT can be effectively treated with antituberculous therapy [38].
Figure 2.
(A): axial T2WI, (B): DWI, (C): NCE FST1WI, (D–F): axial CE dynamic FST1WI (D): pancreatic parenchymal phase, (E): portal venous phase, (F): delayed venous phase, (G): MCRP, (H): coronal T2WI, (I): posttreatment MCRP, (J): posttreatment coronal T2WI. Primary pancreatic tuberculosis in a 15-year-old patient from Burundi presenting with abdominal pain and anicteric cholestasis. Note in the T2WI a hyperintense mass in the head of the pancreas (arrow in (A)) causing an abrupt biliary duct cutoff (arrow in (G)) and upstream dilatation. The mass shows diffusion restriction (arrow in (B)) and progressive enhancement in the dynamic sequences (arrows in (C–F)). EUS-guided FNA revealed necrosis, Langhans giant cells, lymphocytes and macrophages organised in granulomas. Thoracic radiography (not shown) was normal, and diagnosis was primary pancreatic tuberculosis. Both the lesion and mass effect on the common bile duct completely resolved after treatment (I,J).
Figure 2.
(A): axial T2WI, (B): DWI, (C): NCE FST1WI, (D–F): axial CE dynamic FST1WI (D): pancreatic parenchymal phase, (E): portal venous phase, (F): delayed venous phase, (G): MCRP, (H): coronal T2WI, (I): posttreatment MCRP, (J): posttreatment coronal T2WI. Primary pancreatic tuberculosis in a 15-year-old patient from Burundi presenting with abdominal pain and anicteric cholestasis. Note in the T2WI a hyperintense mass in the head of the pancreas (arrow in (A)) causing an abrupt biliary duct cutoff (arrow in (G)) and upstream dilatation. The mass shows diffusion restriction (arrow in (B)) and progressive enhancement in the dynamic sequences (arrows in (C–F)). EUS-guided FNA revealed necrosis, Langhans giant cells, lymphocytes and macrophages organised in granulomas. Thoracic radiography (not shown) was normal, and diagnosis was primary pancreatic tuberculosis. Both the lesion and mass effect on the common bile duct completely resolved after treatment (I,J).

2.3. Solid Serous Cystadenoma (Figure 3)
Solid serous cystadenoma (SSCA) is the rarest variant of pancreatic serous cystadenoma, accounting for only 3% of all cases [39], and with only 22 cases reported in the literature [40]. Serous cystadenomas are benign tumours, usually composed of cysts that can measure up to 2 cm, with a typical honeycomb appearance. A central scar, often calcified, is frequently identified [41].
The solid variant is frequently misdiagnosed, because cystic spaces are either absent or scarce and too tiny [42]. In addition, serous cystadenomas may contain intratumoral haemorrhage, which adds to the high density of these lesions, contributing to the solid appearance. It occurs most commonly in elderly women, as an incidental finding, with no site of preference [40]. If symptomatic, the presentation is usually non-specific, with abdominal pain, abdominal mass and, rarely, jaundice [43].
As the remaining serous cystadenomas, SSCAs are well-delimited lesions, hypointense in T1WIs and hyperintense in T2WIs [44]. Its most salient feature is an early rapid enhancement followed by isointensity in the portal phase, a fact that frequently leads to a misdiagnosis of pNEN [40,45,46]. T2WIs and especially MR cholangiopancreatography (MRCP), a heavily T2WI sequence with an echo time 10 times longer than that of regular T2WIs, help diagnose the hyperintense cyst [47]. A mild dilatation of the pancreatic duct may happen, due to compression.
Preoperative diagnosis is challenging, and aside from pNEN, it is also commonly mistaken for SPT, PM and even PDAC [47].
Once the diagnosis is suspected at cross-sectional imaging, a confirmation by EUS-FNA is achieved in only half of patients [42], as SSCA’s nature may cause the sample to lack the epithelial tissue required for diagnosis.
As in typical serous cystadenomas, surgery is only recommended when causing symptoms, due to compression of neighbouring organs [48] or if diagnosis remains uncertain after workup [43].
Figure 3.
(A): axial NCE-CT, (B): axial CE pancreatic parenchymal phase CT, (C): axial CE portal venous phase CT, (D): axial T2WI-DWI fusion, (E): DWI, (F): ADC, (G): coronal FDG-PET. Solid serous cystadenoma. A 67-year-old patient with fatigue and abdominal pain, referred from another institution with the diagnosis of pancreatic neoplasm. CA 19.9 within normal limits. CT shows a solid lesion in the body of the pancreas (arrow in (A)), with central enhancement in the arterial phase (arrowhead in (B)), which persists during portal phase (arrowhead in (C)). There is no downstream MPD dilatation. Note the diffusion restriction (arrow in (D–F)) and the peripheral hypermetabolic uptake on the PET-CT (arrow in (G)). EUS-guided FNB only obtained inflammatory cells, with no evidence of malignancy. The lesion remained suspicious, and the patient underwent a left pancreatectomy. Histological examination revealed a SSCA.
Figure 3.
(A): axial NCE-CT, (B): axial CE pancreatic parenchymal phase CT, (C): axial CE portal venous phase CT, (D): axial T2WI-DWI fusion, (E): DWI, (F): ADC, (G): coronal FDG-PET. Solid serous cystadenoma. A 67-year-old patient with fatigue and abdominal pain, referred from another institution with the diagnosis of pancreatic neoplasm. CA 19.9 within normal limits. CT shows a solid lesion in the body of the pancreas (arrow in (A)), with central enhancement in the arterial phase (arrowhead in (B)), which persists during portal phase (arrowhead in (C)). There is no downstream MPD dilatation. Note the diffusion restriction (arrow in (D–F)) and the peripheral hypermetabolic uptake on the PET-CT (arrow in (G)). EUS-guided FNB only obtained inflammatory cells, with no evidence of malignancy. The lesion remained suspicious, and the patient underwent a left pancreatectomy. Histological examination revealed a SSCA.

3. Potentially Malignant Lesions (Table S2)
3.1. Solid Pseudopapillary Tumour (Figure 4 and Figure 5)
SPT is a rare pancreatic neoplasm accounting for 2% of all exocrine pancreatic neoplasms [49]. It is an epithelial tumour, but its pathogenesis remains unclear as its cells of origin are unlike any other cell found within the embryonic or adult pancreas [50]. It has been hypothesised that it arises from pluripotential embryonic stem cells [51].
SPT occurs tenfold more frequently in women than in men and this has given origin to a hypothesis linking the tumour to female sex hormones [51,52] or pointing to genital ridges close to the pancreatic anlage during organogenesis as a possible origin [53]. Published cases occurring in men report usually an older age and curiously an aggressive behaviour [54]. Its target populations are women younger than 40 years old [55].
There is no association with a functional endocrine syndrome [56] or with any laboratory finding [57].
This tumour grows at a slow rate, thus it does not cause symptoms and it is incidentally discovered in about 15% of patients [55,56]. When present, symptoms are non-specific [50,55,58]. Jaundice happens very rarely [55]. Hemoperitoneum secondary to tumour rupture, either spontaneous or traumatic [59,60], has been described as a rare presentation.
As a result of its slow growth rate and soft nature, SPT usually presents with a large size at diagnosis (mean size 5 cm) [61].
The tail of the pancreas is a favoured location [50]. An extrapancreatic site of origin is possible, though rare [62,63,64,65,66].
MPD or biliary dilatation almost never occurs [67].
Distant metastases, usually present at the time of diagnosis, occur in about 15% of patients [68] and are predominantly hepatic, peritoneal or lymphatic [68,69,70].
SPT is depicted in cross-sectional images as a homogeneous solid lesion that, as it becomes larger, outgrows the blood supply and suffers degenerative changes. Formation of pseudopapillae occurs as loss of tissue takes place. The stalks of these pseudopapillae contain fragile blood vessels and, as a result, intralesional haemorrhage happens frequently [71,72,73]. All these events contribute to a heterogeneous appearance with variable solid and cystic components and intralesional haemorrhagic and necrotic parts [50]. Intralesional haemorrhagic traces are considered to be pathognomonic findings [74,75]. Internal fluid–fluid levels may also be identified [76]. The different components will be better depicted on MR thanks to its high contrast resolution. A pseudocapsule, reflecting the tumour slow growth, is almost always depictable in tumours larger than 3 cm, granting well-delineated borders. True to its fibrous nature, it is typically hypointense in both T1- and T2WIs and enhances moderately after intravenous contrast injection [76]. Dystrophic calcifications are found in up to 30% of cases [59], with a variety of patterns [77], and occur more frequently in larger tumours [50], as necrotic components fail to reabsorb. Following intravenous contrast administration, SPT shows a heterogeneous nature in the arterial phase, even when small in size, followed by a progressive enhancement in the portal venous phase [78].
Surgical resection may be considered without prior biopsy if the presentation is classic. In atypical presentations, diagnosis is achieved through histological examination following biopsy.
Tumour resection is the treatment with curative intent, with a success rate close to 90% [79]. SPTs usually have a benign behaviour but malignancy has been reported in 10–15% [49,68,70]. Even if metastatic, the prognosis is good, as long an R0 resection is achieved [80]. The only significant proven malignancy predictors are pancreatic duct dilatation, vessel encasement and the presence of metastases [81]. It is extremely important to continue surveillance in the long term, as SPTs are prone to recur and develop metastases as a late event, even years after surgery [82].
Figure 4.
(A): axial T2WI, (B): DWI, (C): ADC, (D): axial NE FST1WI, (E): axial CE portal venous phase FST1WI. Pancreatic solid pseudopapillary tumour in a 20-year-old woman as an incidental finding during a pregnancy check-up. A 10 cm pancreatic mass was found, with a fibrous capsule (arrowhead in (A)), diffusion restriction (arrows in (B,C)) and heterogeneous enhancement (arrow in (D,E)). Imaging findings were compatible with a pancreatic SPT, and it was histologically proven following distal pancreatectomy.
Figure 4.
(A): axial T2WI, (B): DWI, (C): ADC, (D): axial NE FST1WI, (E): axial CE portal venous phase FST1WI. Pancreatic solid pseudopapillary tumour in a 20-year-old woman as an incidental finding during a pregnancy check-up. A 10 cm pancreatic mass was found, with a fibrous capsule (arrowhead in (A)), diffusion restriction (arrows in (B,C)) and heterogeneous enhancement (arrow in (D,E)). Imaging findings were compatible with a pancreatic SPT, and it was histologically proven following distal pancreatectomy.

Figure 5.
(A): axial CE portal venous phase CT, (B): coronal T2WI, (C): MRCP, (D): DWI, (E): ADC, (F): axial NCE FST1WI, (G): axial CE pancreatic parenchymal phase FST1WI, (H): axial CE portal venous phase FST1WI. Pancreatic solid pseudopapillary tumour in a 30-year-old woman as an incidental finding during a CT scan for abdominal pain. CT showed a mass within the body of the pancreas (arrow in (A)). The lesion was well defined by a fibrous capsule (arrowhead in (B)). MPD was displaced, with normal caliber (arrow in (C)). The lesion showed diffusion restriction (arrow in (D,E)) and progressive heterogeneous enhancement (arrow in (F–H)). Due to the microcystic appearance in T2WIs, the lesion was initially thought to be a microcystic serous cystadenoma, even if it lacked some characteristic features. Nevertheless, given its size and presence of symptoms, it was removed. Histological examination revealed a SPT.
Figure 5.
(A): axial CE portal venous phase CT, (B): coronal T2WI, (C): MRCP, (D): DWI, (E): ADC, (F): axial NCE FST1WI, (G): axial CE pancreatic parenchymal phase FST1WI, (H): axial CE portal venous phase FST1WI. Pancreatic solid pseudopapillary tumour in a 30-year-old woman as an incidental finding during a CT scan for abdominal pain. CT showed a mass within the body of the pancreas (arrow in (A)). The lesion was well defined by a fibrous capsule (arrowhead in (B)). MPD was displaced, with normal caliber (arrow in (C)). The lesion showed diffusion restriction (arrow in (D,E)) and progressive heterogeneous enhancement (arrow in (F–H)). Due to the microcystic appearance in T2WIs, the lesion was initially thought to be a microcystic serous cystadenoma, even if it lacked some characteristic features. Nevertheless, given its size and presence of symptoms, it was removed. Histological examination revealed a SPT.

3.2. Pancreatic Schwannoma (Figure 6)
Pancreatic schwannoma (PS) is a rare tumour that arises from Schwann cells found in the sheath of vagus nerve branches on their course through the pancreas [83].
Only 10% of cases are associated with genetic disorders, such as neurofibromatosis type 2 (NF2), multiple meningiomas and schwannomatosis, and, rarely, with neurofibromatosis type 1 (NF1), with an increased risk of malignant transformation [84].
There are less than 80 reported cases in the literature, with most of the cases occurring in adults (average age 55 years), with a slightly higher incidence in women [85].
Patients mostly present with non-specific abdominal complaints [86], although the prevalence of symptoms suspicious for a PDAC (such as weight loss, palpable mass and jaundice) is not neglectable [85].
Levels of CA 19-9 and carcinoembryonic antigen (CEA) are usually within normal values.
Most tumours have been found within the head [87].
Tumour size varies greatly and, with increasing size, there is also proportionate likelihood of degeneration occurring. Microscopically, two distinct areas are found within the tumour: Antoni A, solid, with a compact cellular organisation and a well-developed vascular net, and Antoni B, hypocellular with loose myxoid stroma, less vascularity and degenerative alterations (haemorrhage, calcification, cyst formation, hyalinisation and xanthoma infiltration) [88,89]. The tumour’s appearance is determined by the proportion of Antoni A and B areas; thus, the imaging features are non-specific and preoperative diagnosis is challenging [90].
On CT, benign schwannomas are usually depicted as encapsulated round masses with a variable proportion of avidly enhancing (Antoni A areas) and non-enhancing (Antoni B areas) components, following intravenous contrast administration [91]. On MR, hypointense signal in T1WIs and heterogeneously hyperintense signal in T2WIs are commonly found [92], in addition to progressive enhancement in T1WIs [93].
Suspicious signs of malignancy are rapid growth, invasion of neighbouring structures, a solid inhomogeneous and irregular mass with avid contrast enhancement and associated thrombosis [94].
PS is usually associated with a hypermetabolic appearance on FDG-PET, even if benign [95].
Differential diagnosis should include SPT, pNEN and pancreatic cystadenoma. The diagnosis of PS should be considered when a well-circumscribed lesion with or without a cystic component is encountered, showing increased FDG uptake on PET-CT [95].
Diagnosis is achieved after histological examination following EUS-guided biopsy.
If asymptomatic, a conservative management may be considered, given its benign nature and stable size or slow growth rate [96]. On the other hand, if symptomatic, resection should be considered. Follow-up after surgery should be carried on, as the risk of recurrence remains unknown [97].
Figure 6.
(A): axial T2WI, (B): DWI, (C): ADC, (D): axial CE early arterial phase FST1WI, (E): axial CE pancreatic parenchymal phase FST1WI. Pancreatic schwannoma in a 70-year-old male patient during follow-up for a duodenal gastrointestinal stromal tumour (GIST), removed five years prior through cephalic duodenopancreatectomy. A pancreatic lesion is noted within the pancreatic tail (arrow in (A)). Observe MPD dilatation unrelated to the lesion, due to surgical procedure. The lesion showed diffusion restriction (arrow in (B,C)) and progressive heterogeneous enhancement following intravenous contrast administration (arrow in (D,E)). EUS-guided FNA obtained fragments of mesenchymal tissue with minimal nuclear atypia and positive immunostaining for anti-S-100, and cytological report concluded schwannoma. Tumour board decided conservative management and the lesion is currently under surveillance.
Figure 6.
(A): axial T2WI, (B): DWI, (C): ADC, (D): axial CE early arterial phase FST1WI, (E): axial CE pancreatic parenchymal phase FST1WI. Pancreatic schwannoma in a 70-year-old male patient during follow-up for a duodenal gastrointestinal stromal tumour (GIST), removed five years prior through cephalic duodenopancreatectomy. A pancreatic lesion is noted within the pancreatic tail (arrow in (A)). Observe MPD dilatation unrelated to the lesion, due to surgical procedure. The lesion showed diffusion restriction (arrow in (B,C)) and progressive heterogeneous enhancement following intravenous contrast administration (arrow in (D,E)). EUS-guided FNA obtained fragments of mesenchymal tissue with minimal nuclear atypia and positive immunostaining for anti-S-100, and cytological report concluded schwannoma. Tumour board decided conservative management and the lesion is currently under surveillance.

3.3. Purely Intraductal Pancreatic Neuroendocrine Tumour (Figure 7)
Intraductal growth of a pNEN is encountered in two different scenarios. Most frequently, it is found in the form of a parenchymal lesion that extends into the pancreatic duct and grows along its extent. This presentation is very rare and very few cases have been published [98,99,100,101,102,103,104]. The other, and even rarer, setting is a true intraductal origin, where a NEN arises within the main pancreatic duct as a polypoid mass that grows along the duct [98,105,106] but it is not connected to a parenchymal lesion [107]. Only seven cases of purely intraductal pNENs have been reported in the literature [107]. Purely intraductal pNEN has been hypothesised to rise from totipotential stem cells located within the epithelium of the main duct [108]. As the tumour grows, the tumour may block the duct lumen and, as a result, it can cause pancreatitis. In fact, these tumours frequently present as a chronic pancreatitis. This exclusively intraductal lesion is not conspicuous on CT, and it may be obscured by the pancreatitis signs, so it is most frequently diagnosed after surgery. MRCP proves to be very useful as it can depict the intraductal tumour as a filling defect. Intraductal pNEN may also be identified following intravenous contrast administration as an avidly enhancing lesion in the arterial phase. This type of presentation occurs mostly associated with non-functioning pNENs [107]. An inflammatory stricture in the setting of chronic pancreatitis constitutes the other differential diagnosis possibility. There are so few cases in the literature that no data can be extrapolated.
Figure 7.
(A): MRCP, (B): axial T2WI, (C): DWI, (D): axial CE arterial phase FST1WI. Intraductal pancreatic NEN in a 55-year-old patient with a known history of a testicular tumour, admitted for acute pancreatitis, with no risk factors. Note the marked dilatation of the distal MPD (arrows in (A,B)) with a proximal filling defect (arrowheads in (A,B)) which corresponds to the intraductal tumour. The intraductal mass shows diffusion restriction (arrowhead in (C)) and intense enhancement following intravenous contrast administration (arrowhead in (D)). A total pancreatectomy was decided by the MDT and histological examination concluded grade 2 intraductal pNEN.
Figure 7.
(A): MRCP, (B): axial T2WI, (C): DWI, (D): axial CE arterial phase FST1WI. Intraductal pancreatic NEN in a 55-year-old patient with a known history of a testicular tumour, admitted for acute pancreatitis, with no risk factors. Note the marked dilatation of the distal MPD (arrows in (A,B)) with a proximal filling defect (arrowheads in (A,B)) which corresponds to the intraductal tumour. The intraductal mass shows diffusion restriction (arrowhead in (C)) and intense enhancement following intravenous contrast administration (arrowhead in (D)). A total pancreatectomy was decided by the MDT and histological examination concluded grade 2 intraductal pNEN.

3.4. Pancreatic Solitary Fibrous Tumour (Figure 8)
This type of extrapleural solitary fibrous tumour is a fibroblastic mesenchymal tumour, previously known as haemangiopericytoma. It was first described in the pleura in 1931 [109], derived from mesenchymal cells from pleural connective tissue, but since then, it has been documented in almost every anatomic site, including the retroperitoneum [110].
Pancreatic solitary fibrous tumour (PSFT) is a rare neoplasm, with only 29 cases reported [111]. It shows no gender preference, and the median age reported at diagnosis is 53 years [112]. The main symptoms reported at presentation are abdominal pain and jaundice, though most frequently tumours are incidental findings [113].
Patients may present with refractory and recurrent hypoglucemia as a paraneoplastic syndrome (Doege–Potter syndrome), caused by an increased production of insulin-like growth factor II [113]. Being a mesenchymal tumour, there is no association with tumour markers.
PSFT arises most commonly within the pancreatic head [111].
It shows a true capsule and well-defined margins, and it does not tend to invade the surrounding parenchyma [114]. Its most salient feature is its hypervascularity, and it usually enhances homogeneously and progressively in the arterial and portal phase [115]. In larger tumours, central necrosis occurs, and it has been described that a malignant type may present a heterogeneous appearance with haemorrhage, necrosis and calcifications [115].
Dilatation of the main pancreatic duct has been observed in some cases, as well as biliary dilatation in tumours located within the head [116], but these findings are not a constant, despite the large size of tumours. Lymphadenopathies are not frequently associated [111].
FDG-PET has not been shown to be useful in distinguishing indolent from aggressive PSFT [117], contrary to previous hypotheses.
The main differential diagnosis based on imaging findings is pNEN [118]. Other options should include leiomyosarcoma, GIST, perivascular epithelioid cell tumour (PEComa) and SPT in younger patients.
Definite diagnosis is achieved by EUS-guided biopsy. Curative treatment is complete surgical resection [119], with good results, since most of the published cases were disease free after surgery [115]. Adjuvant radio- or chemotherapy treatments have not achieved successful results [120]. Negative margins have proved to decrease the rate of local recurrence and to improve survival [120]. Follow-up is recommended, as about 12–22% of all solitary fibrous tumours are aggressive, with local recurrence and metastases [121].
Figure 8.
(A): CE-CT portal phase coronal MPR, (B): axial CE arterial phase CT, (C): axial CE portal venous phase CT, (D): FDG-PET CT. Follow-up images (E): axial CE arterial phase FST1WI, (F): axial T2WI. Malignant pancreatic solitary fibrous tumour in a 47-year-old patient who presented with a palpable mass within the right hypochondrium. She had a history of a nasal fibrous solitary tumour 10 years prior. CT showed an enormous solid mass in the head of the pancreas, causing mild dilatation of the pancreatic duct (arrow in (A)). Note the central necrosis (* in (C)) and the hypervascularity of the non-necrotic periphery (arrow in (B)), which is highly metabolic on the FDG-PET (arrow in (D)). The patient underwent a total pancreatectomy and the histological examination concluded PSFT. It turned out to have a malignant outcome and the patient developed liver (arrow in (E)) and omental (arrow in (F)) metastases within the year following the surgery.
Figure 8.
(A): CE-CT portal phase coronal MPR, (B): axial CE arterial phase CT, (C): axial CE portal venous phase CT, (D): FDG-PET CT. Follow-up images (E): axial CE arterial phase FST1WI, (F): axial T2WI. Malignant pancreatic solitary fibrous tumour in a 47-year-old patient who presented with a palpable mass within the right hypochondrium. She had a history of a nasal fibrous solitary tumour 10 years prior. CT showed an enormous solid mass in the head of the pancreas, causing mild dilatation of the pancreatic duct (arrow in (A)). Note the central necrosis (* in (C)) and the hypervascularity of the non-necrotic periphery (arrow in (B)), which is highly metabolic on the FDG-PET (arrow in (D)). The patient underwent a total pancreatectomy and the histological examination concluded PSFT. It turned out to have a malignant outcome and the patient developed liver (arrow in (E)) and omental (arrow in (F)) metastases within the year following the surgery.

4. Malignant Lesions (Table S3)
4.1. Acinar Cell Carcinoma (Figure 9 and Figure 10)
Acinar cell carcinoma is a rare epithelial malignant primary pancreatic tumour, named after the acinar differentiation of its cells. Even though acinar cells constitute most of the pancreatic parenchyma, acinar cell carcinoma (ACC) paradoxically represents less than 2% of primary pancreatic neoplasms [122].
ACC occurs mostly in men (men to women ratio of 3.6) with a bimodal presentation, with two incidence peaks at 8–15 and 60 years [123,124,125].
It arises throughout the pancreas, with no favoured location.
Presenting symptoms are non-specific, with abdominal pain and weight loss being the most common. Pancreatitis and obstructive jaundice are rare [126,127] as, despite their large size, ACCs do not tend to cause ductal obstruction [128,129].
Elevated lipase, secreted by the tumour, may be the presenting sign of ACC and may be used as a tumour marker [130]. As a result, fat necrosis may be triggered, either subcutaneously, presenting as nodules, or within the cancellous bone, causing polyarthralgia [131,132]. These symptoms, together with peripheral eosinophilia, constitute a paraneoplastic syndrome [133] that may occur after tumour recurrence. An elevated alpha-fetoprotein may sometimes be found [134]. Levels of CA 19-9 and carcinoembryonic antigen (CEA) are usually within normal values.
At the time of presentation, almost half of patients present with hepatic and lymph node metastases [135].
On cross-sectional imaging, ACC usually appears as a large (average size at diagnosis of 10cm [136,137,138]), well-defined and oval or round exophytic mass (it may even be found attached to the surface of the pancreas on the histological examination [130]). Calcifications are found in one third of patients [136,137,139]. It usually shows a solid appearance, but internal haemorrhage, necrosis and cystic changes are common in larger lesions [136]. On unenhanced CT, it is usually iso-hypodense to the pancreatic parenchyma, and it shows a hypovascular nature, hypoenhancing in the arterial phase and becoming more enhancing than the pancreatic parenchyma in the portal venous phase [140]. An enhancing capsule may also be identified.
Concerning the cross-sectional imaging test of choice, the combination of CT and MR works well in depicting the imaging features. MR outperforms CT in describing tumour limits, intratumoral bleeding, local invasion and ductal dilatation, whereas CT is better at detecting calcification [141].
Differential diagnosis should include PDAC, pNENs, SPT and, in children, also pancreatoblastoma. PDAC usually shows a smaller size with no calcification or cystic changes [142]. Its margins are not well delineated, and invasion of neighbouring structures is one of its hallmarks. ACCs are often mistaken for large pNENs, as they may show heterogeneous density/SI due to haemorrhage, necrosis, cystic changes and calcifications, but ACCs are mainly hypovascular. SPTs may also mimic ACCs, but the target population is the key: they occur almost exclusively in young women, in which ACCs rarely occur [143]. Pancreatoblastoma may cause a differential diagnosis issue, as it usually occurs in infants and children [144]. Its frequently also presents with liver metastases, but it is more aggressive than ACC.
Even if almost half of patients present at diagnosis with hepatic and regional lymph nodes metastases [135,145], ACC shows a better prognosis than PDAC, with a 5-year survival rate of 50% [146,147]. However, ACC has a higher rate of recurrence [141].
Surgical resection with negative margins is the only therapeutic approach that improves long-term survival. Recent studies suggest that the outcome of combining surgery and chemotherapy is more favourable than that of only surgery [148].
Figure 9.
(A): axial T2WI, (B): MRCP following secretin injection, (C): axial T2 DWI fusion, (D): ADC, (E): axial CE pancreatic parenchymal phase FST1WI, (F): axial CE portal venous phase FST1WI. Acinar cell adenocarcinoma in a 79-year-old patient with previous episodes of pancreatitis of unknown cause and elevated lipase in current laboratory results. A solid well-defined mass (arrow in (A)) with lobulated contours and minimal MPD stenosis (* in (A)) is found in the distal pancreas. It shows diffusion restriction (arrows in (C,D)). Note the duct penetrating sign following secretin injection (arrow in (B)). It is hypoenhancing in the early arterial phase (arrow in (E)) with progressive enhancement during pancreatic parenchymal phase (arrow in (F)). No adenopathies are found. Findings were non-specific and did not fulfill the diagnosis criteria for PDAC. Diagnosis was achieved at histological examination following EUS-guided FNB.
Figure 9.
(A): axial T2WI, (B): MRCP following secretin injection, (C): axial T2 DWI fusion, (D): ADC, (E): axial CE pancreatic parenchymal phase FST1WI, (F): axial CE portal venous phase FST1WI. Acinar cell adenocarcinoma in a 79-year-old patient with previous episodes of pancreatitis of unknown cause and elevated lipase in current laboratory results. A solid well-defined mass (arrow in (A)) with lobulated contours and minimal MPD stenosis (* in (A)) is found in the distal pancreas. It shows diffusion restriction (arrows in (C,D)). Note the duct penetrating sign following secretin injection (arrow in (B)). It is hypoenhancing in the early arterial phase (arrow in (E)) with progressive enhancement during pancreatic parenchymal phase (arrow in (F)). No adenopathies are found. Findings were non-specific and did not fulfill the diagnosis criteria for PDAC. Diagnosis was achieved at histological examination following EUS-guided FNB.

Figure 10.
(A): axial T2WI, (B): DWI, (C): ADC, (D): CE pancreatic parenchymal phase FST1WI, (E): axial CE portal venous phase FST1WI, (F): axial CE delayed venous phase FST1WI. Acinar cell adenocarcinoma incidentally discovered in a 70-year-old female patient during a routine echography. Note the lesion within the head of the pancreas, rather exophytic and heterogeneous (arrow in (A)), with diffusion restriction (arrows in (B,C)). During the dynamic sequences following intravenous contrast administration (arrows in (D–F)), the lesion shows capsular enhancement while the center remains hypointense, due to necrosis/cystic changes. Due to its exophytic appearance, the lesion was thought to be within the pancreaticoduodenal groove and, hence, was diagnosed as a GIST. Histopathological examination following EUS-guided FNB revealed an ACC.
Figure 10.
(A): axial T2WI, (B): DWI, (C): ADC, (D): CE pancreatic parenchymal phase FST1WI, (E): axial CE portal venous phase FST1WI, (F): axial CE delayed venous phase FST1WI. Acinar cell adenocarcinoma incidentally discovered in a 70-year-old female patient during a routine echography. Note the lesion within the head of the pancreas, rather exophytic and heterogeneous (arrow in (A)), with diffusion restriction (arrows in (B,C)). During the dynamic sequences following intravenous contrast administration (arrows in (D–F)), the lesion shows capsular enhancement while the center remains hypointense, due to necrosis/cystic changes. Due to its exophytic appearance, the lesion was thought to be within the pancreaticoduodenal groove and, hence, was diagnosed as a GIST. Histopathological examination following EUS-guided FNB revealed an ACC.

4.2. Undifferentiated Carcinoma with Osteoclastic-like Giant Cells (Figure 11)
Undifferentiated carcinoma with osteoclastic-like giant cells (UCOGC) is an extremely rare and aggressive subtype of pancreatic adenocarcinoma. It constitutes less than 1% of all pancreatic malignant tumours [149].
Its histogenesis is not clear, as at the time of diagnosis, it presents with a large size and its relation to the pancreatic duct is difficult to establish. About 20% of cases seem to arise from mucinous or intraductal papillary mucinous neoplasms (IPMNs) [150] and it has been hypothesised that it has an epithelial origin with a mesenchymal transition [150,151]. The epithelial to mesenchymal transition is a transient and reversible transformation which is normally activated during embryonic development and tissue repair but also during carcinogenesis [152,153]. Through this step, tumoral cells acquire mesenchymal features that enable them to invade adjacent vessels and distant organs [154].
Two phenotypes have been described [155], a pure form containing only osteoclast-like giant cells, with a better prognosis than the mixed form, a combination of undifferentiated carcinoma of the pancreas and osteoclast-like giant cells forming a very aggressive tumour with a poor outcome. This mixed form constitutes a distinct variant from undifferentiated carcinoma of the pancreas [156]. UCOGC may occur in association with PDAC [157].
UCOGC occurs more commonly in women (women:men ratio of 13:8) with higher prevalence in middle-aged and elderly patients [158].
Presenting symptoms are non-specific and consist of upper abdominal pain, weight loss and/or anorexia. Jaundice and steatorrhoea have been described in 25% of cases [159].
CA 19-9 and CEA serum levels have been reported to be increased in some patients [160].
Favoured locations are the body and tail of the pancreas [157].
Biliary ducts and pancreatic duct dilatation may occur [151,158,159], as UCOGC seems prone to grow intraductally [151].
At presentation, UCOGCs are usually large lesions [161], locally aggressive, with a tendency to invade adjacent structures. Lymph node involvement and distant metastases are rarely encountered [151,161].
On cross-sectional imaging, appearance may vary and it displays non-specific features, either hypovascular [158] or hypervascular [162]. Hypervascular behaviour may be explained by a relationship to giant cell tumours of the bone, also hypervascular, so enhancement is proportionate to the volume of the osteoclastic cell component [151]. Haemorrhage [163], cystic changes [162], necrosis [158] calcification [164] and vascular invasion may occur [163].
UCOGC may be misdiagnosed as PDAC, mucinous carcinoma [165], SPT [158], pNEN [166] and pancreatic pseudocyst [167].
Diagnosis follows histological examination after EUS biopsy. Surgical resection is the treatment of choice. The efficacy of chemotherapy and radiotherapy has not been proved yet.
Its prognosis is variable, ranging from a few months to up to ten years as reported in the literature [168]. It was traditionally considered worse than that of PDAC [169,170] due to the advanced stage at diagnosis [165] and its tendency to recur even after complete resection [165,171].
Another analysis result of another series concluded that the prognosis (5-year survival >50%) is considerably better than that of PDAC [150]. It has been hypothesised that these discordant prognosis results are probably due to the use of wrong terminology [172] and it is clear that true UCOGCs have a more indolent behaviour [164], especially the pure form [173].
The underlying reasons for the better prognosis compared to PDAC may be its slower local spread, more indolent nature, better response to surgery and/or chemotherapy, less nodal involvement and fewer distant metastases [174].
The most important criterion for prognosis is the presence of an associated PDAC [173].
Figure 11.
(A): axial FST2WI, (B): MRCP, (C): DWI, (D): ADC, (E): NEC axial FST1WI, (F): axial CE pancreatic parenchymal phase FST1WI, (G): axial CE portal venous phase FST1WI. UCOGC in a 45-year-old patient who presented with bloating. A cephalic pancreatic mass was identified, hyperintense in T2WIs (arrow in (A)), with MPD integrity (arrow in (B)) and no biliary duct dilatation, diffusion restriction (arrows in (C,D)) and scarce progressive enhancement in the dynamic sequences (arrows in (E–G)). These non-specific features did not fulfil PDAC diagnostic criteria. Ascites (* in (G)) and peritoneal deposits (arrow in (G)) were also found. Histology examination following EUS-guided FNB revealed a UCOGC.
Figure 11.
(A): axial FST2WI, (B): MRCP, (C): DWI, (D): ADC, (E): NEC axial FST1WI, (F): axial CE pancreatic parenchymal phase FST1WI, (G): axial CE portal venous phase FST1WI. UCOGC in a 45-year-old patient who presented with bloating. A cephalic pancreatic mass was identified, hyperintense in T2WIs (arrow in (A)), with MPD integrity (arrow in (B)) and no biliary duct dilatation, diffusion restriction (arrows in (C,D)) and scarce progressive enhancement in the dynamic sequences (arrows in (E–G)). These non-specific features did not fulfil PDAC diagnostic criteria. Ascites (* in (G)) and peritoneal deposits (arrow in (G)) were also found. Histology examination following EUS-guided FNB revealed a UCOGC.

4.3. Pancreatic Adenosquamous Carcinoma (Figure 12)
Pancreatic adenosquamous carcinoma (PASC) is a rare and aggressive variant of PDAC which is frequently misdiagnosed as such on imaging or even histopathologically. Its actual prevalence is thus inexact and has been reported to range from 0.38 to 10% [175,176,177]. A squamous cell component of at least 30% among glandular elements of PDAC has been a requisite for the diagnosis [178,179], although the required percentage recently has been questioned, as the proportion of squamous carcinoma does not have a clinical correlation and its evaluation remains subjective [180,181,182,183].
As squamous cells are not found in normal pancreatic tissue, the pathophysiology remains a mystery. Three hypotheses have been reported. The leading theory proposes that since squamous cells are found in the setting of chronic pancreatitis or in the event of tumour ductal obstruction and these conditions are associated with PDAC, squamous carcinoma could arise from a preexisting adenocarcinoma, through metaplastic changes [179,181,184,185]. PASC could also be the result of two different neoplastic pancreatic cell lines merging [184,186,187] or even having a common origin, as the third theory implies, where certain pluripotential primitive cells would differentiate into adenocarcinoma and others into squamous cell carcinoma, resulting in a tumour with both cell types [179,184].
Squamous carcinoma tends to show intercellular bridges and/or focal keratin pearl formation within its cells. However, PASC frequently presents as a poorly differentiated tumour and the use of immunochemistry is often needed to confirm the differentiation [188].
Elevated levels of CA 19-9 and CEA are found in most patients [189]. Hypercalcemia of malignancy is found in some cases, probably related to high serum levels of parathyroid hormone-related protein [190,191,192].
There is a higher prevalence in men and average age at presentation is 68 years [175].
Presenting symptoms are non-specific and indistinguishable from those of PDAC (abdominal pain, weight loss, anorexia and jaundice) [186,193].
Most frequently, at presentation, PASC is locally advanced or has distant metastases [194]: liver, lung [195,196] and even bone and skin [197,198,199].
Like PDAC, the head of the pancreas is the most common location but it arises within the body–tail more often than PDAC [175].
It is frequently associated with MPD dilatation and CBD dilatation when found within the head.
PASC tends to be larger than PDAC. It appears as a round lobulated mass with extensive central necrosis which causes an hyperintensity in T2WIs greater than that of PDAC [200] and a fibrous capsule that enhances progressively. Enhancement is overall considered to be greater than that of PDAC [201]. Another presenting imaging feature which may be helpful to distinguish it from PDAC is the frequently associated portal vein tumour thrombus [189,201,202,203].
Diagnosis may be achieved presurgically through an EUS-guided biopsy.
Complete resection is the only potentially curative treatment, although only 15–20% of patients are surgical candidates. A less favourable outcome has traditionally been associated with PASC, compared to PDAC, with a worse survival in patients who have undergone resection [204]. However, surgical resection has been shown to significantly improve median patient survival: median overall survival after surgery is 12 months, while in PDAC it is 16 months [175]. On the other end of the differentiation spectrum, squamous cell carcinoma appears to be an even more aggressive tumour, with worse survival data, which might suggest that the squamous element is a worsening prognosis factor [204].
Figure 12.
(A): axial NCE-CT, (B): axial CE pancreatic parenchymal phase CT, (C): axial CE portal venous phase CT, (D): CE portal phase CT coronal MPR. Adenosquamous carcinoma. A 60-year-old patient with elevated liver enzymes was discovered to have a pancreatic mass during an ultrasound. Note the subtle contour abnormalities of the pancreatic head on the unenhanced CT (arrow in (A)) and the progressively enhancing lesion (arrow in (B,C)). Observe the biliary duct (arrow in (D)) and the upstream MPD dilatation (arrowhead in (D)). EUS-guided FNA concluded moderately differentiated adenocarcinoma and, since the tumour was resectable, the patient underwent surgery. Histological examination proved it to be a PASC. Retrospectively, it shows a greater enhancement than a typical PDAC.
Figure 12.
(A): axial NCE-CT, (B): axial CE pancreatic parenchymal phase CT, (C): axial CE portal venous phase CT, (D): CE portal phase CT coronal MPR. Adenosquamous carcinoma. A 60-year-old patient with elevated liver enzymes was discovered to have a pancreatic mass during an ultrasound. Note the subtle contour abnormalities of the pancreatic head on the unenhanced CT (arrow in (A)) and the progressively enhancing lesion (arrow in (B,C)). Observe the biliary duct (arrow in (D)) and the upstream MPD dilatation (arrowhead in (D)). EUS-guided FNA concluded moderately differentiated adenocarcinoma and, since the tumour was resectable, the patient underwent surgery. Histological examination proved it to be a PASC. Retrospectively, it shows a greater enhancement than a typical PDAC.

4.4. Colloid Carcinoma (Figure 13)
Colloid carcinoma (CC) of the pancreas, alternatively referred to as mucinous non-cystic carcinoma, is a rare variant of ductal adenocarcinoma, which occurs with a rate of 1% of all pancreatic tumours [205,206].
Its hallmark is the abundant presence of extracellular mucin (adding up to at least 50% of the tumour), with malignant cells floating within it [207]. This mucinous component is the reason why it was previously categorised as mucinous cystadenoma or signet-ring cell carcinoma of the pancreas [206].
It appears that there is a slightly higher prevalence in men [205,208,209] and age at presentation ranges within the seventh decade [205].
Tumour markers (including CEA and CA 19-9) are usually elevated [205].
Presenting symptoms resemble those associated with PDAC: abdominal pain, jaundice and weight loss [179]. Almost half of patients with CC present a history of pancreatitis [209].
Most colloid carcinomas are associated with intestinal-type invasive IPMN although they may also arise de novo [210,211], and these types occur most frequently within the head of the pancreas [211,212]. Another less frequent association has been described with mucinous cystic tumours, involving preferably the tail of the pancreas [205].
CC is a slow-growing tumour that shows local invasion rather than disseminated disease [212]. Lymph node metastases and vascular invasion occur less frequently in CC than in PDAC [213,214].
The presence of dilatation of the main pancreatic duct will depend on whether the CC derives from an IPMN; if so, the tumour will be intraluminal, either the main or branch duct, and there will be downstream MPD dilatation [213]. If the tumour is unrelated to an IPMN, no dilatation will be found. Bile duct dilatation may occur in tumours arising from the head of the pancreas.
The reported tumour size at presentation ranges from 1 to 16cm [205,206]. Usually, they present on CT with a lobulated appearance and slightly ill-defined margins [215]. Calcifications are often found [215]. In T2WIs, CC shows very bright signal intensity with internal septa and a salt and pepper appearance, these features being consistent with the abundant mucin lakes with floating stroma and tumour cells [210]. Enhancement will happen typically progressively so at a delayed phase it will be more conspicuous. Enhancement will be observed internally in a sponge-like fashion, due to the enhancing stroma amidst the mucin lakes, which will enhance poorly and peripherally, associated with induced desmoplastic reaction [210,215].
CC has an indolent behaviour, and its prognosis is superior to PDAC: 5-year survival rates of 40–60% vs. 10–15%, respectively [216,217]. One of the reasons explaining this better prognosis is the mucin, which surrounds the cells and acts as a barrier preventing their spread [207,216]. The other reason lies within the surface glycoproteins present in colloid carcinoma: MUC1 is present in PDAC on the luminal aspect or throughout the cells, whereas CC expresses MUC1 on the basal surface [218]. Also, another surface glycoprotein found in CC, MUC2, not found in PDAC, has been described to have tumour suppressor activity [215].
A misleading cystic appearance due to the abundant mucin production may cause a misdiagnosis of cystic tumours, such as IPMN or a mucinous cystic adenocarcinoma [219]. Hallmarks to distinguish IPMN-unrelated colloid carcinomas from IPMN in cross-sectional images are an absence of communication with the MPD and of intraductal papillary components and a lack of downstream pancreatic ductal dilatation, features that can be successfully assessed with MRCP. Also, the typical papillary bulging into the duodenal lumen and spillage of mucin from the ampulla of Vater, typical findings on endoscopic retrograde cholangiopancreatography (ERCP), will not be present in CC [210,220]. Mucinous cystic adenocarcinomas, on the other hand, are large well-defined unilocular or macrocystic lesions with enhancing soft tissue components, different from the not-so-well-defined CC with progressive internal enhancement, besides the fact that the target populations are women.
In the event of an intraluminal CC communicating with the MPD, features will be difficult to distinguish from invasive IPMN on cross-sectional imaging and ERCP will be essential to rule IPMN out.
Even though FNA is useful to describe the large amounts of mucin, it may not provide enough data to complete the diagnosis [221]. The presence of malignant epithelial cells within a mucin magma should provide definitive diagnosis [179]. However, given the rarity of this entity, CCs are typically diagnosed during histological examination following surgery.
Surgery is recommended as the only curative treatment in eligible patients [221]. A recent study has suggested that adjuvant chemotherapy may not be effective for CC [222]. The survival rate has been reported to be better than for PDAC (5-year survival rate of 57%) [223]. Long-term surveillance is recommended to detect recurrence [221].
Figure 13.
(A): axial CE portal venous phase CT, (B): axial T2WI, (C): coronal T2WI, (D): MRCP, (E): DWI, (F): ADC, (G): axial NCE FST1WI, (H): CE pancreatic parenchymal phase FST1WI, (I): axial CE portal venous phase FST1WI. Colloid carcinoma. Patient is a 52-year-old woman with left upper quadrant pain for the previous six months and weight loss (15 kg). Blood laboratory tests are anodyne. Observe the intraluminal mass within the body and distal pancreas (* in (A–D)), notice its salt and pepper pattern in T2WIs (* in (B,C)) and how it is partly calcified (arrowhead in (A)). The lesion is associated with downstream MPD dilatation (arrow in (A,B,D)) and side branch ecstasy (arrowhead in (C,D)). There is no diffusion restriction (arrow in (E,F)). In the dynamic sequences following intravenous contrast administration, the tumour shows gradual enhancement of the periphery and the subtle septa (arrows in (G–I)). Patient underwent a cephalic duodenopancreatectomy and diagnosis was pathologically proven.
Figure 13.
(A): axial CE portal venous phase CT, (B): axial T2WI, (C): coronal T2WI, (D): MRCP, (E): DWI, (F): ADC, (G): axial NCE FST1WI, (H): CE pancreatic parenchymal phase FST1WI, (I): axial CE portal venous phase FST1WI. Colloid carcinoma. Patient is a 52-year-old woman with left upper quadrant pain for the previous six months and weight loss (15 kg). Blood laboratory tests are anodyne. Observe the intraluminal mass within the body and distal pancreas (* in (A–D)), notice its salt and pepper pattern in T2WIs (* in (B,C)) and how it is partly calcified (arrowhead in (A)). The lesion is associated with downstream MPD dilatation (arrow in (A,B,D)) and side branch ecstasy (arrowhead in (C,D)). There is no diffusion restriction (arrow in (E,F)). In the dynamic sequences following intravenous contrast administration, the tumour shows gradual enhancement of the periphery and the subtle septa (arrows in (G–I)). Patient underwent a cephalic duodenopancreatectomy and diagnosis was pathologically proven.

4.5. Primary Pancreatic Leiomyosarcoma (Figure 14 and Figure 15)
Primary pancreatic leiomyosarcoma (PPLM) belongs to the group of malignant mesenchymal tumours that may originate in the pancreas, along with malignant peripheral nerve sheath tumours, undifferentiated pleomorphic sarcomas, liposarcomas, rhabdomyosarcomas, solitary fibrous tumour and primitive neuroectodermal tumours (PNETs), among which it ranks first in frequency [224]. It is a very rare and aggressive tumour, which accounts only for 0.1% of malignant pancreatic neoplasms [225].
Its cells show smooth muscle features [226], a fact that has given rise to theories regarding the walls of intrapancreatic vessels or the smooth muscle cells of the pancreatic ducts as possible origins [226]. These theories may be the rationale behind the close relationship between the tumour and the vessels/duct [226,227,228,229].
It occurs most frequently during the fifth decade; gender predominance is not clear [226,230,231,232]. An association with East Asian ethnicity has been recently proposed, with a higher prevalence of regional invasion [233].
Presenting symptoms are non-specific and variable, and the most frequently encountered complaints are abdominal pain/tenderness, weight loss and a palpable abdominal mass [229].
Since it is a mesenchymal tumour, there is no association with tumour markers.
No preferred site within the pancreas has been described [226], and there is similar incidence between the head and the body–tail [232].
It is locally very aggressive and, since it is usually discovered at a late stage, invasion of neighbouring organs and vessels is a frequent feature. It is prone to metastasise to the liver, and lung metastases are also frequently present at diagnosis [232,234]. However, lymphatic spread is rare [226,229], a fact that could be helpful for differential diagnosis.
PPLMs have been described in the literature as non-specific masses on CT/MR, with size ranging from 3–25cm [230], that, as volume increases, become heterogeneous, with haemorrhagic, necrotic and cystic components, due to degenerative changes [232,235]. Peripheric enhancement is present with a large central non-enhancing component [235,236]. These features may lead to misdiagnosis of a large leiomyosarcoma as a pseudocyst [229] or a cystoadenocarcinoma [237].
Usually, there is no associated MPD dilatation. However, tumours arising from smooth cells of the pancreatic duct have been described [238].
It has been proposed that diagnosis should be entertained when confronted with a mass that fulfils the following criteria: large size, increased enhancement and absence of biliary duct dilatation [236] and other authors have added the presence of cystic/necrotic components to the list [239,240].
Differential diagnosis includes the far more frequent PDAC, and, less frequently, pNEN [240,241,242], a metastasis to the pancreas from another known primary tumour [240,243] and, more rarely, an invading leiomyosarcoma originating from adjacent organs and simulating a pancreatic primary tumour [244]. An isolated metastasis to the pancreas from a distant leiomyosarcoma is extremely rare [245], with female genital tract, gastrointestinal tract, soft tissues of the extremities and retroperitoneum as most common sites of origin [246].
Diagnosis is usually achieved after histological examinations and immunohistochemical staining [232], following surgery or intraoperative biopsy. EUS-guided FNA often comes up with false negative results due to the cystic and fibrous nature of the lesion [235,247].
In the absence of organ/vessel invasion or distant metastases, radical resection with negative margins stands as the only potentially curative treatment [248].
Radiation and chemotherapy have not achieved clinical success, as for other leiomyosarcomas [249,250,251].
It is usually associated with a poor outcome; the median survival time in a series of 49 cases [252] was 48 months.
Figure 14.
(A): axial CE portal venous phase CT, (B): axial T2WI, (C): DWI, (D): ADC, (E): axial CE pancreatic parenchymal phase FST1WI, (F): axial CE portal venous phase FST1WI. Primary pancreatic leiomyosarcoma incidentally discovered in a 53-year-old patient during a routine check-up. Note the heterogeneous mass within the pancreatic isthmus (arrow in (B)) with compression of the superior mesenteric and splenic vein (arrow in (A)). No biliary or pancreatic duct dilatation is observed. The lesion shows diffusion restriction (arrow in (C,D)) and hypervascularity, with progressive enhancement following intravenous contrast administration (arrow in (E,F)). EUS-guided FNB concluded PPLM. The patient underwent radiotherapy before surgery but then refused to be operated upon and developed hepatic and muscular metastases (not shown here). Stable disease was achieved with chemotherapy for five years, but it is currently progressing.
Figure 14.
(A): axial CE portal venous phase CT, (B): axial T2WI, (C): DWI, (D): ADC, (E): axial CE pancreatic parenchymal phase FST1WI, (F): axial CE portal venous phase FST1WI. Primary pancreatic leiomyosarcoma incidentally discovered in a 53-year-old patient during a routine check-up. Note the heterogeneous mass within the pancreatic isthmus (arrow in (B)) with compression of the superior mesenteric and splenic vein (arrow in (A)). No biliary or pancreatic duct dilatation is observed. The lesion shows diffusion restriction (arrow in (C,D)) and hypervascularity, with progressive enhancement following intravenous contrast administration (arrow in (E,F)). EUS-guided FNB concluded PPLM. The patient underwent radiotherapy before surgery but then refused to be operated upon and developed hepatic and muscular metastases (not shown here). Stable disease was achieved with chemotherapy for five years, but it is currently progressing.

Figure 15.
(A): axial T2WI, (B): DWI, (C): ADC, (D): axial NCE FST1WI, (E): axial CE pancreatic parenchymal phase FST1WI, (F): axial CE portal venous phase FST1WI. Primary pancreatic leiomyosarcoma incidentally discovered in a 50-year-old female patient during an ultrasound for a urinary infection. Observe the large heterogeneous mass in T2WI (arrow in (A)) within the distal pancreas, with diffusion restriction (arrow in (B,C)). The sequences following intravenous contrast administration show the central cystic/necrotic component (* in (E,F)) and the solid and progressively peripheral enhancement (arrow in (D–F)). Resectability criteria were fulfilled, and patient underwent distal pancreatectomy. Histological examination concluded PPLM.
Figure 15.
(A): axial T2WI, (B): DWI, (C): ADC, (D): axial NCE FST1WI, (E): axial CE pancreatic parenchymal phase FST1WI, (F): axial CE portal venous phase FST1WI. Primary pancreatic leiomyosarcoma incidentally discovered in a 50-year-old female patient during an ultrasound for a urinary infection. Observe the large heterogeneous mass in T2WI (arrow in (A)) within the distal pancreas, with diffusion restriction (arrow in (B,C)). The sequences following intravenous contrast administration show the central cystic/necrotic component (* in (E,F)) and the solid and progressively peripheral enhancement (arrow in (D–F)). Resectability criteria were fulfilled, and patient underwent distal pancreatectomy. Histological examination concluded PPLM.

4.6. Primary and Secondary Pancreatic Lymphoma (Figure 16, Figure 17 and Figure 18)
Primary pancreatic lymphoma (PPL) is an extremely rare non-epithelial tumour that accounts for less than 0.5% of all pancreatic tumours and 1% of all extranodal lymphomas [253].
PPL occurs most commonly in middle-aged patients (mean age 53 years) [254], especially Caucasians [255], and with a male prevalence [254]. It is frequently associated with immunosuppression that seems to favour the disease [256].
Patients mainly complain of abdominal pain at diagnosis. Other presenting symptoms are jaundice, which is relatively common, pancreatitis and/or gastric or duodenal obstruction [110,257]. Fever, chills, night sweats and weight loss are associated with systemic non-Hodgkin lymphoma (constituting the classic B symptoms) but are rare in PPL [254].
The most frequent subtype is B-cell non-Hodgkin lymphoma [255].
CA 19-9 usually ranges within normal limits [254], even though PPL-associated biliary dilatation may cause a mild elevation of CA 19-9 [252]; LDH is often elevated [256]. Thus, the combination of increased LDH serum levels without concurrent increased CA 19-9 should favour the diagnosis of pancreatic lymphoma [255,258].
Different morphologic patterns have been described [259], the most common is a solitary focal mass. A diffuse infiltration with pancreatic enlargement, a peripheral involvement and a multinodular type comprehend the rest of the presentations.
The focal pattern occurs mainly within the head, as the part that contains the largest concentration of lymphoid tissue [255,260]. It is depicted as a bulky, well-circumscribed mass, ranging between 2 and 14 cm [255]. It is homogeneous, and it shows progressive and delayed but limited homogeneous enhancement, to a lesser degree compared to the preserved pancreatic parenchyma [259]. Characteristically, necrosis and calcification are hardly ever present [261], although necrosis may happen secondary to concomitant acute pancreatitis, or due to a duodenal fistula causing an intratumoral collection [262]. Compared to the preserved pancreatic parenchyma, PPL is usually hypointense in T1WIs and hyperintense in T2WIs [262]. The hallmark on MR imaging is the significant diffusion restriction, similar to that of the spleen.
The infiltrative pattern leads to a diffuse, ill-defined enlargement of the pancreas and may mimic acute pancreatitis [263]. However, even if both the focal and diffuse patterns may be associated with stranding of the peripancreatic fat [264], it is minimal, unlike the marked inflammation associated with acute pancreatitis. Moreover, the typical peripancreatic collections and a concordant clinical history are absent.
Peripheral involvement occurs rarely, as a focally enlarged hypointense pancreas in T1- and T2WIs, and with a capsule-like rim, which may mimic autoimmune pancreatitis [265].
The multinodular pattern is similar to the solitary focal mass, but the lesions are smaller [254]. Differential diagnosis includes multiple metastases from hypovascular tumours and multifocal autoimmune pancreatitis.
Despite the large size previously mentioned, the main pancreatic duct is usually not dilated [254] and pancreatic atrophy is not present [264]. Nevertheless, mild pancreatic duct dilatation may still be found so its presence should not rule out the possibility of pancreatic lymphoma [261]. The biliary duct has been described for a considerable number of patients [261]. However, even if present, biliary and/or pancreatic ductal obstruction will be disproportionately milder than expected, considering the size of the mass.
As with lymphomas elsewhere, PPL may infiltrate surrounding organs, not respecting anatomic boundaries, and may displace and encase adjacent vessels but will not invade or cause stenosis or occlusion [254]. No irregularities within the vessel wall are found [257,258].
A small volume of retroperitoneal lymphadenopathy is frequently found to be associated, both peripancreatic and around the aorta and cava vein. If present below the renal veins, pancreatic ductal adenocarcinoma can be confidently excluded [259,266,267].
Secondary pancreatic lymphoma (SPL) is a direct involvement of the pancreas from peripancreatic adenopathies and, as opposed to the primary tumour, occurs more frequently, in up to 30% of lymphoma patients [257], especially in widespread nodal or extranodal disease [268]. Even in this scenario, a predominant involvement of the pancreas is quite uncommon [269]. The most common type is diffuse large B-cell non-Hodgkin lymphoma [270]. SPL may also show the different presentation patterns previously described [259]. It may be difficult to distinguish on imaging from the diffuse form of PPL, but the clinical setting is different.
PPL may be misdiagnosed as PDAC, as they share imaging features. Differentiation becomes critical as PPL is highly sensitive to chemotherapy and does not require surgery. Diagnosis is achieved after EUS-guided biopsy. Long-term regression or remission is frequently achieved, with survival rates similar to those of nodal non-Hodgkin lymphoma [255]. However, relapses occur frequently [271], especially at distant sites, like the central nervous system [255,257,272], and prolonged follow-up is recommended.
Figure 16.
(A,B): axial CE portal venous phase CT. (C): axial FST2WI, (D): DWI, (E): ADC, (F): axial NCE FST1WI, (G): axial CE pancreatic parenchymal phase FST1W1, (H): axial CE portal venous phase FST1W1. Primary pancreatic lymphoma (focal form) in a 26-year-old patient with obstructive jaundice. CT revealed a hypovascular mass in the head of the pancreas (thin arrows in (A,B)), with minimal bile (arrowhead in (A)) and MPD dilatation (thick arrow in (A)), no distal parenchymal atrophy and abutment of the superior mesenteric vein (arrowhead in (B)). Note in the T2WI a homogeneous slightly hyperintense mass (arrow in (C)) with marked diffusion restriction (arrows in (D,E)) and its hypovascularity following intravenous contrast administration. Considering the tumour size, its homogeneity, marked diffusion restriction, growth pattern and hypovascularity with minimal MPD and biliary dilatation, lymphoma was one of the top possibilities on the differential diagnosis list. Note a small haematoma in the center of the mass (arrows on (F–H)) secondary to a EUS-guided biopsy, which concluded Burkitt lymphoma. The patient was successfully treated with chemotherapy, obtaining a complete remission.
Figure 16.
(A,B): axial CE portal venous phase CT. (C): axial FST2WI, (D): DWI, (E): ADC, (F): axial NCE FST1WI, (G): axial CE pancreatic parenchymal phase FST1W1, (H): axial CE portal venous phase FST1W1. Primary pancreatic lymphoma (focal form) in a 26-year-old patient with obstructive jaundice. CT revealed a hypovascular mass in the head of the pancreas (thin arrows in (A,B)), with minimal bile (arrowhead in (A)) and MPD dilatation (thick arrow in (A)), no distal parenchymal atrophy and abutment of the superior mesenteric vein (arrowhead in (B)). Note in the T2WI a homogeneous slightly hyperintense mass (arrow in (C)) with marked diffusion restriction (arrows in (D,E)) and its hypovascularity following intravenous contrast administration. Considering the tumour size, its homogeneity, marked diffusion restriction, growth pattern and hypovascularity with minimal MPD and biliary dilatation, lymphoma was one of the top possibilities on the differential diagnosis list. Note a small haematoma in the center of the mass (arrows on (F–H)) secondary to a EUS-guided biopsy, which concluded Burkitt lymphoma. The patient was successfully treated with chemotherapy, obtaining a complete remission.

Figure 17.
(A): axial CE portal venous phase CT, (B): axial T2WI, (C): FDG-PET-CT. Primary pancreatic lymphoma (diffuse form) in a 65-year-old alcoholic patient referred to our institution after being diagnosed with a pancreatic mass. An ill-defined infiltrating pancreatic mass is observed (arrow in (A)), with no biliary or pancreatic duct dilatation (observe the MPD’s normal appearance, arrow in (B)). The mass shows an intense hypermetabolic uptake on the FDG-PET-CT (arrow in (C)). Biopsy revealed a high-grade PPL with diffuse big cell B lymphoma and Burkitt-like components.
Figure 17.
(A): axial CE portal venous phase CT, (B): axial T2WI, (C): FDG-PET-CT. Primary pancreatic lymphoma (diffuse form) in a 65-year-old alcoholic patient referred to our institution after being diagnosed with a pancreatic mass. An ill-defined infiltrating pancreatic mass is observed (arrow in (A)), with no biliary or pancreatic duct dilatation (observe the MPD’s normal appearance, arrow in (B)). The mass shows an intense hypermetabolic uptake on the FDG-PET-CT (arrow in (C)). Biopsy revealed a high-grade PPL with diffuse big cell B lymphoma and Burkitt-like components.

Figure 18.
Images from 2017, (A,B): axial and coronal CE portal venous phase CT MPR. Images from 2022, (C,D): axial and coronal CE portal venous phase CT MPR. Secondary pancreatic lymphoma in a 60-year-old patient with a known glomus jugulotympanicum paraganglioma on surveillance. Note the normal appearance of pancreas and the spleen (A,B) on the prior CT. Abdominal adenopathies were found (not shown). Observe the spleen enlargement (arrow in (D)), with focal lesions. Hepatoduodenal and retroperitoneal adenopathies were also found (not shown). Note the isoenhancing mass within the body of the pancreas (arrow in (C)). EUS-guided FNB revealed a diffuse large B-cell SPL.
Figure 18.
Images from 2017, (A,B): axial and coronal CE portal venous phase CT MPR. Images from 2022, (C,D): axial and coronal CE portal venous phase CT MPR. Secondary pancreatic lymphoma in a 60-year-old patient with a known glomus jugulotympanicum paraganglioma on surveillance. Note the normal appearance of pancreas and the spleen (A,B) on the prior CT. Abdominal adenopathies were found (not shown). Observe the spleen enlargement (arrow in (D)), with focal lesions. Hepatoduodenal and retroperitoneal adenopathies were also found (not shown). Note the isoenhancing mass within the body of the pancreas (arrow in (C)). EUS-guided FNB revealed a diffuse large B-cell SPL.

4.7. Pancreatic Metastases (Figure 19, Figure 20, Figure 21 and Figure 22)
Metastases to the pancreas are uncommon, only accounting for 2–5% of pancreatic malignancies [273]. They mostly occur secondary to intra-abdominal tumours [274], including RCC, colon and gastric cancer [275,276], although lung cancer also ranks high among the most frequent sites of origin [276].
PM may invade the epithelium of the pancreatic duct and mimic PDAC symptoms, namely, jaundice and abdominal pain as the most common presenting signs [276,277]. However, PM may also be asymptomatic and incidentally identified during the initial workup of the primary tumour or during surveillance. There may be a latency period from the diagnosis of the primary tumour to the detection of PM, which in the case of clear cell renal or breast carcinoma may be quite long, up to 21 years after surgery of RCC [276,277,278].
PMs are commonly associated with widespread disease, at a late stage, and more than 90% of patients have extrapancreatic disease [279]. However, it should be noted that in more than half of PM cases, the pancreas is the only organ metastatically involved [280], especially in RCC [281].
There is no location predilection within the pancreas [282]. In the particular case of PM from lung cancers, the head seems to be a favoured site as 76% of small cell lung carcinomas, the histological type mostly associated with PM [283], arise there [284].
Cancer antigens have little diagnostic reliability [285]. In an analysis of series with 192 cases in total, CA 19-9 was elevated in 8–28% of cases, but this may be related to the gastrointestinal origin of most of the primary tumours included and unrelated to PM [286].
Three patterns of metastatic involvement have been described. The most common appearance (50–75%) is the single pattern, depicting a solitary, localised and well-defined lesion. The second most common is the diffuse infiltration that causes a generalised enlargement of the pancreas (15–44%). The remaining pattern (5–10%) is represented by several nodules, which can coalesce into larger masses [280,287].
Dilatation of the main pancreatic or bile ducts is uncommon [288].
PMs typically appear hypointense in FST1WIs compared to normal parenchyma and may show moderate hyperintensity in T2WIs [289] although they may also appear hypointense, especially in the diffuse infiltration pattern. The behaviour after intravenous contrast injection relates to size: even though most of the lesions are hypovascular, lesions smaller than 1.5 cm may be hypervascular and larger lesions may show a rim of enhancement due to central necrosis [290,291]. This peripheral enhancement pattern has been described as a frequent finding (41%) [263,292], especially in PMs from RCC. The rationale behind this enhancement pattern is that the periphery of the lesion receives more blood than the center, since PMs nurture themselves by parasitising blood supply from the surrounding parenchyma.
As in any other organ, PM features resemble those of the primary tumour, e.g., PMs from RCC are often hypervascular [293]. PMs from melanoma, due to the paramagnetic effect of melanin, show a high signal intensity in T1WIs and low signal intensity in T2WIs [294]. PMs from dermatofibrosarcoma are usually hypointense in T1WIs, slightly hyperintense in T2WIs and show a spoke wheel-like enhancement [295].
At least one third of PMs are misdiagnosed as primary tumours [296]. Differential diagnosis of hypervascular PM should include primary pancreatic NET, intrapancreatic accessory spleen and vascular lesions [292]. Hypovascular PMs need to be differentiated from PDAC, lymphoma and focal pancreatitis [297,298]. Peripheral enhancement is a useful sign to differentiate PM from PDAC [263]; other distinguishing features are absence of dilatation of the upstream pancreatic duct and/or bile ducts, parenchymal atrophy and absence of vessel involvement [293,294].
The treatment of choice in eligible patients is pancreatic metastasectomy. However, its success depends on the biology of the primary tumour. According to most large studies, the best long-term survival predictor is the type of cancer [275,299]. PMs from RCC achieve the best outcome (61% 5-year survival) [274] and surgery is the treatment of choice if all metastatic lesions can be resected, although there is a high rate of recurrence (33–42% of patients who undergo pancreatic metastasectomy). On the other end of the spectrum, lung carcinoma is associated with the worst survival (0%) [300].
Figure 19.
(A): axial CE-CT, (B): coronal MPR CE portal venous phase CT, (C): axial T2WI, (D): MRCP, (E): DWI, (F): ADC, (G): axial NCE FST1WI, (H): axial CE arterial phase FST1WI, (I): axial CE portal venous phase FST1WI. Solitary PM from lung adenocarcinoma in a 56-year-old patient with advanced stage disease and hyperbilirubinemia. Observe the primary tumour within the left hilum (arrow in (A)). The patient also presented peritoneal and bone metastases, not shown. A mass was found within the head of the pancreas (arrowhead in (B)), with no MPD dilatation (arrowhead in (C)). However, the lesion was associated with discreet common bile duct dilatation (arrow in (D)). Observe the diffusion restriction (arrowhead in (E,F)) and the progressive peripheral enhancement following intravenous contrast administration (arrowhead in (G–I)) with central necrosis. Note the resemblance to the primary tumour (arrow in (A)). EUS-guided FNB confirmed a PM from an adenocarcinoma of pulmonary origin.
Figure 19.
(A): axial CE-CT, (B): coronal MPR CE portal venous phase CT, (C): axial T2WI, (D): MRCP, (E): DWI, (F): ADC, (G): axial NCE FST1WI, (H): axial CE arterial phase FST1WI, (I): axial CE portal venous phase FST1WI. Solitary PM from lung adenocarcinoma in a 56-year-old patient with advanced stage disease and hyperbilirubinemia. Observe the primary tumour within the left hilum (arrow in (A)). The patient also presented peritoneal and bone metastases, not shown. A mass was found within the head of the pancreas (arrowhead in (B)), with no MPD dilatation (arrowhead in (C)). However, the lesion was associated with discreet common bile duct dilatation (arrow in (D)). Observe the diffusion restriction (arrowhead in (E,F)) and the progressive peripheral enhancement following intravenous contrast administration (arrowhead in (G–I)) with central necrosis. Note the resemblance to the primary tumour (arrow in (A)). EUS-guided FNB confirmed a PM from an adenocarcinoma of pulmonary origin.

Figure 20.
(A): axial CE-CT, (B): axial T2WI, (C): DWI, (D): ADC, (E): axial NCE FST1W1, (F): axial CE arterial phase FST1W1. Solitary PM from a known RCC discovered during follow-up in a 56-year-old patient who underwent a right nephrectomy 10 years prior. A homogeneous mass was found within the body of the pancreas (arrow in (A,B)), with discrete pancreatic duct dilatation and distal parenchymal atrophy (arrowhead in (A)). The mass showed diffusion restriction (arrow in (C,D)) and marked peripheral enhancement (arrow in (E,F)). An EUS-guided FNB showed rare epithelial cells and concluded haemorrhagic cyst. Given the discordance between the images and the histological report, the MDT decided to perform a left pancreatectomy and the histological examination concluded RCC metastasis.
Figure 20.
(A): axial CE-CT, (B): axial T2WI, (C): DWI, (D): ADC, (E): axial NCE FST1W1, (F): axial CE arterial phase FST1W1. Solitary PM from a known RCC discovered during follow-up in a 56-year-old patient who underwent a right nephrectomy 10 years prior. A homogeneous mass was found within the body of the pancreas (arrow in (A,B)), with discrete pancreatic duct dilatation and distal parenchymal atrophy (arrowhead in (A)). The mass showed diffusion restriction (arrow in (C,D)) and marked peripheral enhancement (arrow in (E,F)). An EUS-guided FNB showed rare epithelial cells and concluded haemorrhagic cyst. Given the discordance between the images and the histological report, the MDT decided to perform a left pancreatectomy and the histological examination concluded RCC metastasis.

Figure 21.
(A): axial T2WI, (B): DWI, (C): ADC, (D): NCE FST1W1, (E): CE arterial phase FST1W1 subtraction, (F): CE portal venous phase FST1W1 subtraction. PM from a known malignant skin melanoma in a 54-year-old patient who presented with acute abdominal pain. A heterogeneous mass was found within the body of the pancreas (arrow in (A)), showing diffusion restriction (arrow in (B,C)) and no pancreatic duct dilatation. The lesion showed hyperintense content in T1WIs (arrowhead in (D)) compatible with melanin, with scarce enhancement after intravenous contrast administration (arrow in (E,F)). There were also several melanin-containing hepatic lesions (* in (D)). Diagnosis of pancreatic and hepatic metastases was proven by biopsy.
Figure 21.
(A): axial T2WI, (B): DWI, (C): ADC, (D): NCE FST1W1, (E): CE arterial phase FST1W1 subtraction, (F): CE portal venous phase FST1W1 subtraction. PM from a known malignant skin melanoma in a 54-year-old patient who presented with acute abdominal pain. A heterogeneous mass was found within the body of the pancreas (arrow in (A)), showing diffusion restriction (arrow in (B,C)) and no pancreatic duct dilatation. The lesion showed hyperintense content in T1WIs (arrowhead in (D)) compatible with melanin, with scarce enhancement after intravenous contrast administration (arrow in (E,F)). There were also several melanin-containing hepatic lesions (* in (D)). Diagnosis of pancreatic and hepatic metastases was proven by biopsy.

Figure 22.
(A): image from 2016: coronal CE T1WI. Images from 2021: (B): axial T2WI, (C): DWI, (D): ADC, (E): NCE FST1WI, (F–H): axial CE dynamic FST1WI (pancreatic parenchymal, portal venous and delayed venous phase). PM from a facial DFSP in a 35-year-old patient who presented with elevated pancreatic enzymes on a check-up, five years after the primary tumour diagnosis (arrow in (A)). Five solid lesions were found within the pancreas, of which only one is shown, slightly hyperintense in T2WIs (arrow in (B)) with minimal MPD dilatation (arrowhead in (B)), diffusion restriction (arrow in (C,D)) and a hypovascular behaviour following intravenous contrast administration with progressive enhancement (corresponding to the fibrous content) (arrow in (E–H)). Histological examination following EUS-FNB concluded PM from DFSP.
Figure 22.
(A): image from 2016: coronal CE T1WI. Images from 2021: (B): axial T2WI, (C): DWI, (D): ADC, (E): NCE FST1WI, (F–H): axial CE dynamic FST1WI (pancreatic parenchymal, portal venous and delayed venous phase). PM from a facial DFSP in a 35-year-old patient who presented with elevated pancreatic enzymes on a check-up, five years after the primary tumour diagnosis (arrow in (A)). Five solid lesions were found within the pancreas, of which only one is shown, slightly hyperintense in T2WIs (arrow in (B)) with minimal MPD dilatation (arrowhead in (B)), diffusion restriction (arrow in (C,D)) and a hypovascular behaviour following intravenous contrast administration with progressive enhancement (corresponding to the fibrous content) (arrow in (E–H)). Histological examination following EUS-FNB concluded PM from DFSP.

5. Conclusions
Several rare focal and diffuse lesions may be found in the pancreas, either incidentally discovered, related to specific or, most frequently, non-specific clinical symptoms and biological abnormalities, or in the setting of a known oncologic condition. These lesions are associated with different behaviours, which range from benign to very aggressively malignant and, therefore, they are associated with different prognosis. Cross-sectional imaging findings combined with the clinico-biological setting contribute substantially to achieving the correct diagnosis. Typical imaging features related to the appearance of the lesion on cross-section imaging modalities in addition to indirect associated signs, such as the presence/absence of biliary and/or pancreatic duct dilatation, invasion of adjacent organs, peripancreatic vascular involvement or loco-regional lymph nodal invasion together with the presence of distant metastases, are crucial to correctly address the diagnosis.
Nevertheless, challenging cases occur, in which imaging features remain indeterminate and there is no typical clinical or biological presentation, and thus EUS-FNA/FNB is required to obtain histologically proven confirmation of the nature of the lesion, which is mandatory for optimal patient management.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics13162719/s1, Table S1: Benign Lesions; Table S2: Potentially Malignant Lesions; Table S3: Malignant Lesions.
Funding
This review received no external funding.
Acknowledgments
The authors are grateful to Valérie Vilgrain for contributing with the colloid carcinoma case and Pedro Veron Guembe for his help with editing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fletcher, J.G.; Wiersema, M.J.; Farrell, M.A.; Fidler, J.L.; Burgart, L.J.; Koyama, T.; Johnson, C.D.; Stephens, D.H.; Ward, E.M.; Harmsen, W.S. Pancreatic malignancy: Value of arterial, pancreatic, and hepatic phase imaging with multi-detector row CT. Radiology 2003, 229, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Dodds, W.J.; Taylor, A.J.; Erickson, S.J.; Stewart, E.T.; Lawson, T.L. Radiologic imaging of splenic anomalies. AJR Am. J. Roentgenol. 1990, 155, 805–810. [Google Scholar] [CrossRef]
- Lehtinen, S.J.; Schammel, C.M.; Devane, M.; Trocha, S.D. Intrapancreatic accessory spleen presenting as a pancreatic mass. J. Gastrointest. Oncol. 2013, 4, E23–E26. [Google Scholar]
- Lake, S.T.; Johnson, P.T.; Devane, M.; Trocha, S.D. CT of splenosis: Patterns and pitfalls. AJR Am. J. Roentgenol. 2012, 199, W686–W693. [Google Scholar] [CrossRef] [PubMed]
- White, J.D.; West, A.N.; Priebat, D.A. Splenosis mimicking an intra-abdominal malignancy. Am. J. Med. 1989, 87, 687–690. [Google Scholar] [CrossRef]
- Abu Hilal, M.; Harb, A.; Zeidan, B.; Steadman, B.; Primrose, J.N.; Pearce, N.W. Hepatic splenosis mimicking HCC in a patient with hepatitis C liver cirrhosis and mildly raised alpha feto protein; the important role of explorative laparoscopy. World J. Surg. Oncol. 2009, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.; Ren, Z.; Da Rold, A.; Guerriero, S.; Pariset, S.; Buffone, A.; Tedeschi, U. A rare diagnosis for a pancreatic mass: Splenosis. J. Gastrointest. Surg. 2004, 8, 915–916. [Google Scholar]
- Halpert, B.; Gyorkey, F. Lesions observed in accessory spleens of 311 patients. Am. J. Clin. Pathol. 1959, 32, 165–168. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, J.M.; Han, J.K.; Lee, J.Y.; Kim, K.W.; Cho, K.C.; Choi, B.I. Intrapancreatic accessory spleen: Findings on MR Imaging, CT, US and scintigraphy, and the pathologic analysis. Korean J. Radiol. 2008, 9, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Varga, I.; Galfiova, P.; Adamkov, M.; Danisovic, L.; Polak, S.; Kubikova, E.; Galbavy, S. Congenital anomalies of the spleen from an embryological point of view. Med. Sci. Monit. 2009, 15, RA269–RA276. [Google Scholar] [PubMed]
- Kawamoto, S.; Johnson, P.T.; Hall, H.; Cameron, J.L.; Hruban, R.H.; Fishman, E.K. Intrapancreatic accessory spleen: CT appearance and differential diagnosis. Abdom. Imaging 2012, 37, 812–827. [Google Scholar] [CrossRef]
- Glazer, G.M.; Axel, L.; Goldberg, H.I.; Moss, A.A. Dynamic CT of the normal spleen. AJR Am. J. Roentgenol. 1981, 137, 343–346. [Google Scholar] [CrossRef]
- Ding, Q.; Ren, Z.; Wang, J.; Ma, X.; Zhang, J.; Sun, G.; Zuo, C.; Gu, H.; Jiang, H. Intrapancreatic accessory spleen: Evaluation with CT and MRI. Exp. Ther. Med. 2018, 16, 3623–3631. [Google Scholar] [CrossRef]
- Lin, W.C.; Lee, R.C.; Chiang, J.H.; Wei, C.J.; Chu, L.S.; Liu, R.S.; Chang, C.Y. MR features of abdominal splenosis. AJR Am. J. Roentgenol. 2003, 180, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Davidson, E.D.; Campbell, W.G.; Hersh, T. Epidermoid splenic cyst occurring in an intrapancreatic accessory spleen. Dig. Dis. Sci. 1980, 25, 964–967. [Google Scholar] [CrossRef]
- Hu, S.; Zhu, L.; Song, Q.; Chen, K. Epidermoid cyst in intrapancreatic accessory spleen: Computed tomography findings and clinical manifestation. Abdom. Imaging 2012, 37, 828–833. [Google Scholar] [CrossRef]
- Okura, N.; Mori, K.; Morishita, Y.; Oda, T.; Tanoi, T.; Minami, M. Inflammatory pseudotumor of the intrapancreatic accessory spleen: Computed tomography and magnetic resonance imaging findings. Jpn. J. Radiol. 2012, 30, 171–175. [Google Scholar] [CrossRef]
- Mariani, G.; Bruselli, L.; Kuwert, T.; Kim, E.E.; Flotats, A.; Israel, O.; Dondi, M.; Watanabe, N. A review on the clinical uses of SPECT/CT. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1959–1985. [Google Scholar] [CrossRef]
- Barquilla-Cordero, P.; Chiquero-Palomo, M.; Martín-Noguerol, E.; Pacheco-Gómez, N.; Vinagre-Rodríguez, G.; Moyano-Calvente, S.L.; Molina-Infante, J. Tuberculosis pancreática primaria en un paciente inmunocompetente: Primer caso comunicado en España. Gastroenterol. Hepatol. 2010, 33, 582–585. [Google Scholar] [CrossRef]
- Panic, N.; Maetzel, H.; Bulajic, M.; Radovanovic, M.; Löhr, J.-M. Pancreatic tuberculosis: A systematic review of symptoms, diagnosis and treatment. United Eur. Gastroenterol. J. 2020, 8, 396–402. [Google Scholar] [CrossRef]
- De Backer, A.I.; Mortelé, K.J.; Bomans, P.; De Keulenaer, B.L.; Vanschoubroeck, I.J.; Kockx, M.M. Tuberculosis of the pancreas: MRI features. AJR Am. J. Roentgeno 2005, 184, 50–54. [Google Scholar] [CrossRef]
- Pandita, K.K.; Sarla, D.S. Isolated pancreatic tuberculosis. Indian. J. Med. Microbiol. 2009, 27, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Baraboutis, I.; Skoutelis, A. Isolated tuberculosis of pancreas. J. Pancreas 2004, 5, 155–158. [Google Scholar]
- Xia, F.; Poon, R.T.; Wang, S.G.; Bie, P.; Huang, X.Q.; Dong, J.H. Tuberculosis of pancreas and peripancreatic lymph nodes in immunocompetent patients: Experience from China. World J. Gastroenterol. 2003, 9, 1361–1364. [Google Scholar] [CrossRef] [PubMed]
- Nagar, A.M.; Raut, A.A.; Morani, A.C.; Sanghvi, D.A.; Desai, C.S.; Thapar, V.B. Pancreatic Tuberculosis: A Clinical and Imaging Review of 32 Cases. J. Comput. Assist. Tomogr. 2009, 33, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Knowles, K.F.; Saltman, D.; Robson, H.G.; Lalonde, R. Tuberculous pancreatitis. Tubercle 1990, 71, 65–68. [Google Scholar] [CrossRef]
- Radin, D.R. Intraabdominal Mycobacterium tuberculosis vs Mycobacterium avium-intracellulare infections in patients with AIDS: Distinction based on CT findings. AJR Am. J. Roentgenol. 1991, 156, 487–491. [Google Scholar] [CrossRef]
- Tetlezi, J.P.; Pisegna, J.R.; Barkin, J.S. Tuberculous pancreatic abscess as a manifestation of AIDS. Am. J. Gastroenterol. 1989, 84, 581–582. [Google Scholar]
- Levine, R.; Tenner, S.; Steinberg, W.; Ginsberg, A.; Borum, M.; Huntington, D. Tuberculous abscess of the pancreas. Case report and review of literature. Dig. Dis. Sci. 1992, 37, 141–144. [Google Scholar] [CrossRef]
- Puri, R.; Thandassery, R.B.; Eloubeidi, M.A.; Sud, R. Diagnosis of isolated pancreatic tuberculosis: The role of EUS-guided FNA cytology. Gastrointest. Endosc. 2012, 75, 900–904. [Google Scholar] [CrossRef]
- Pombo, F.; Díaz Candamio, M.J.; Rodriguez, E.; Pombo, S. Pancreatic tuberculosis. CT findings. Abdom. Imaging 1998, 23, 394–397. [Google Scholar] [CrossRef]
- Ladas, S.D.; Vaidakis, E.; Lariou, C.; Anastasiou, K.; Chalevelakis, G.; Kintzonidis, D.; Raptis, S.A. Pancreatic tuberculosis in non-immunocompromised patients: Reports of two cases and a literature review. Eur. J. Gastroenterol. Hepatol. 1998, 10, 973–976. [Google Scholar] [CrossRef]
- Dou, Y.; Liang, Z. Pancreatic tuberculosis: A computed tomography imaging review of thirteen cases. Radiol. Infect. Dis. 2019, 6, 31–37. [Google Scholar] [CrossRef]
- Fischer, G.; Spengler, U.; Nuebrand, M.; Sauerbruch, T. Isolated tuberculosis of the pancreas masquerading as a pancreatic mass. Am. J. Gastroenterol. 1995, 90, 2227–2230. [Google Scholar]
- Rana, S.S.; Sharma, V.; Sampath, S.; Sharma, R.; Mittal, B.R.; Bhasin, D.K. Vascular invasion does not discriminate between pancreatic tuberculosis and pancreatic malignancy: A case series. Ann. Gastroenterol. 2014, 27, 395–398. [Google Scholar]
- Sharma, V.; Rana, S.S.; Kumar, A.; Bhasin, D.K. Pancreatic tuberculosis. J. Gastroenterol. Hepatol. 2016, 31, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, G.F.; Al-Nakshabandi, N.A. Pancreatic tuberculosis: Role of multidetector computed tomography. Can. Assoc. Radiol. J. 2011, 62, 260–264. [Google Scholar] [CrossRef]
- D’Cruz, S.; Sachdev, A.; Kaur, L.; Handa, U.; Bhalla, A.; Lehl, S.S. Fine needle aspiration diagnosis of isolated pancreatic tuberculosis. A case report and review of literature. J. Pancreas 2003, 4, 158–162. [Google Scholar]
- Kimura, W.; Moriya, T.; Hirai, I.; Hanada, K.; Abe, H.; Yanagisawa, A.; Fukushima, N.; Ohike, N.; Shimizu, M.; Hatori, T.; et al. Multicenter study of serous cystic neoplasm of the Japan pancreas society. Pancreas 2012, 41, 380–387. [Google Scholar] [CrossRef]
- Demesmaker, V.; Abou-Messaoud, F.; Parent, M.; Vanhoute, B.; Maassarani, F.; Kothonidis, K. Pancreatic solid serous cystadenoma: A rare entity that can lead to a futile surgery. J. Surg. Case Rep. 2019, 12, 360. [Google Scholar] [CrossRef]
- Compagno, J.; Oertel, J.E. Microcystic adenoma of the pancreas (glycogen-rich cystadenoma): A clinicopathologic study of 34 cases. Am. J. Clin. Pathol. 1978, 69, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.C.; Singhi, A.D.; Haroun, R.R.; Hruban, R.H.; Fishman, E.K. The many faces of pancreatic serous cystadenoma: Radiologic and pathologic correlation. Diagn. Interv. Imaging 2017, 98, 191–202. [Google Scholar] [CrossRef]
- Jais, B.; Rebours, V.; Malleo, G.; Salvia, R.; Fontana, M.; Maggino, L.; Bassi, C.; Manfredi, R.; Moran, R.; Lennon, A.M.; et al. Serous cystic neoplasm of the pancreas: A multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut 2016, 65, 305–312. [Google Scholar] [CrossRef]
- Okumura, Y.; Noda, T.; Eguchi, H.; Iwagami, Y.; Yamada, D.; Asaoka, T.; Kawamoto, K.; Gotoh, K.; Kobayashi, S.; Umeshita, K.; et al. Middle segment pancreatectomy for a solid serous cystadenoma diagnosed by MRCP and review of the literature: A case report. Mol. Clin. Oncol. 2018, 8, 675–682. [Google Scholar] [CrossRef]
- Kishida, Y.; Matsubayashi, H.; Okamura, Y.; Uesaka, K.; Sasaki, K.; Sawai, H.; Imai, K.; Ono, H. A case of solid-type serous cystadenoma mimicking neuroendocrine tumor of the pancreas. J. Dig. Dis. 2014, 15, 211–215. [Google Scholar] [CrossRef]
- Sun, H.Y.; Kim, S.H.; Kim, M.A.; Lee, J.Y.; Han, J.K.; Choi, B.I. CT imaging spectrum of pancreatic serous tumors: Based on new pathologic classification. Eur. J. Radiol. 2010, 75, 45–55. [Google Scholar] [CrossRef]
- Stern, J.R.; Frankel, W.L.; Ellison, E.C.; Bloomston, M. Solid serous microcystic adenoma of the pancreas. World J. Surg. Oncol. 2007, 5, 26. [Google Scholar] [CrossRef]
- European Study Group on Cystic Tumours of the Pancreas: European evidence-based guidelines on pancreatic cystic neoplasms. Gut 2018, 67, 789–804. [CrossRef] [PubMed]
- Ganeshan, D.M.; Paulson, E.; Tamm, E.P.; Taggart, M.W.; Balachandran, A.; Bhosale, P. Solid pseudo-papillary tumors of the pancreas: Current update. Abdom. Imaging 2013, 38, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- De Robertis, R.; Marchegiani, G.; Catania, M.; Ambrosetti, M.C.; Capelli, P.; Salvia, R.; D’Onofrio, M. Solid Pseudopapillary Neoplasms of the Pancreas: Clinicopathologic and Radiologic Features According to Size. AJR Am. J. Roentgenol. 2019, 213, 1073–1080. [Google Scholar] [CrossRef]
- Canzonieri, V.; Berretta, M.; Buonadonna, A.; Libra, M.; Vasquez, E.; Barbagallo, E.; Bearz, A.; Berretta, S. Solid pseudopapillary tumour of the pancreas. Lancet Oncol. 2003, 4, 255–256. [Google Scholar] [CrossRef] [PubMed]
- Cienfuegos, J.A.; Lozano, M.D.; Rotellar, F.; Martí, P.; Pedano, N.; Arredondo, J.; Bellver, M.; Sola, J.J.; Pardo, F. Solid pseudopapillary tumor of the pancreas (SPPT). Still an unsolved enigma. Rev. Esp. Enferm. Dig. 2010, 102, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Kosmahl, M.; Seada, L.S.; Jänig, U.; Harms, D.; Klöppel, G. Solid-pseudopapillary tumor of the pancreas: Its origin revisited. Virchows Arch. 2000, 436, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.C.; Machado, M.A.; Bacchella, T.; Jukemura, J.; Almeida, J.L.; Cunha, J.E. Solid pseudopapillary neoplasm of the pancreas: Distinct patterns of onset, diagnosis, and prognosis for male versus female patients. Surgery 2008, 143, 29–34. [Google Scholar] [CrossRef]
- Papavramidis, T.; Papavramidis, S. Solid pseudopapillary tumors of the pancreas: Review of 718 patients reported in English literature. J. Am. Coll. Surg. 2005, 200, 965–972. [Google Scholar] [CrossRef]
- Orlando, C.A.; Bowman, R.L.; Loose, J.H. Multicentric papillary-cystic neoplasm of the pancreas. Arch. Pathol. Lab. Med. 1991, 115, 958–960. [Google Scholar]
- Salvia, R.; Bassi, C.; Festa, L.; Falconi, M.; Crippa, S.; Butturini, G.; Brighenti, A.; Capelli, P.; Pederzoli, P. Clinical and biological behavior of pancreatic solidpseudopapillary tumors: Report on 31 consecutive patients. J. Surg. Oncol. 2007, 95, 304–310. [Google Scholar] [CrossRef]
- Adams, A.L.; Siegal, G.P.; Jhala, N.C. Solid pseudopapillary tumor of the pancreas: A review of salient clinical and pathologic features. Adv. Anat. Pathol. 2008, 15, 39–45. [Google Scholar] [CrossRef]
- Huang, S.C.; Wu, T.H.; Chen, C.C.; Chen, T.C. Spontaneous rupture of solid pseudopapillary neoplasm of the pancreas during pregnancy. Obs. Gynecol. 2013, 121, 486–488. [Google Scholar] [CrossRef]
- Mirapoğlu, S.L.; Aydogdu, I.; Gucin, Z.; Yilmaz, T.F.; Umutoglu, T.; Kilincaslan, H. Traumatic rupture of solid pseudopapillary tumors of the pancreas in children: A case report. Mol. Clin. Oncol. 2016, 5, 587–589. [Google Scholar] [CrossRef]
- Hibi, T.; Ojima, H.; Sakamoto, Y.; Kosuge, T.; Shimada, K.; Sano, T.; Sakamoto, M.; Kitajima, M.; Yamasaki, S. A solid pseudopapillary tumor arising from the greater omentum followed by multiple metastases with increasing malignant potential. J. Gastroenterol. 2006, 41, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zong, L.; Wang, P.; Liu, Y.; Zhang, H.; Chang, X.; Lu, Z.; Li, W.; Ma, Y.; Yu, S.; et al. Solid Pseudopapillary Neoplasms of the Pancreas: Clinicopathologic Analysis and a Predictive Model. Mod. Pathol. 2023, 36, 100141. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Huang, Y.F.; Liu, X.H.; Xu, M.H. Extrapancreatic solid pseudopapillary neoplasm followed by multiple metastases: Case report. World J. Gastrointest. Oncol. 2017, 9, 497–501. [Google Scholar] [CrossRef]
- Miyazaki, Y.; Miyajima, A.; Maeda, T.; Yuge, K.; Hasegawa, M.; Kosaka, T.; Kikuchi, E.; Kameyama, K.; Jinzaki, M.; Nakagawa, K.; et al. Extrapancreatic solid pseudopapillary tumor: Case report and review of the literature. Int. J. Clin. Oncol. 2012, 17, 165–168. [Google Scholar] [CrossRef]
- Deshpande, V.; Oliva, E.; Young, R.H. Solid pseudopapillary neoplasm of the ovary: A report of 3 primary ovarian tumors resembling those of the pancreas. Am. J. Surg. Pathol. 2010, 34, 1514–1520. [Google Scholar] [CrossRef] [PubMed]
- Walter, T.; Hommell-Fontaine, J.; Hervieu, V.; Adham, M.; Poncet, G.; Dumortier, J.; Lombard-Bohas, C.; Scoazec, J.Y. Primary malignant solid pseudopapillary tumors of the gastroduodenal area. Clin. Res. Hepatol. Gastroenterol. 2011, 35, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Buetow, P.C.; Buck, J.L.; Pantongrag-Brown, L.; Beck, K.G.; Ros, P.R.; Adair, C.F. Solid and papillary epithelial neoplasm of the pancreas: Imaging-pathologic correlation on 56 cases. Radiology 1996, 199, 707–711. [Google Scholar] [CrossRef]
- Alexandrescu, D.T.; O’Boyle, K.; Feliz, A.; Fueg, A.; Wiernik, P.H. Metastatic solid-pseudopapillary tumour of the pancreas: Clinico-biological correlates and management. Clin. Oncol. 2005, 17, 358–363. [Google Scholar] [CrossRef]
- Lee, J.H.; Yu, J.S.; Kim, H.; Kim, J.K.; Kim, T.H.; Kim, K.W.; Park, M.S.; Kim, J.H.; Kim, Y.B.; Park, C. Solid pseudopapillary carcinoma of the pancreas: Differentiation from benign solid pseudopapillary tumour using CT and MRI. Clin. Radiol. 2008, 63, 1006–1014. [Google Scholar] [CrossRef]
- Hassan, I.; Celik, I.; Nies, C.; Zielke, A.; Gerdes, B.; Moll, R.; Ramaswamy, A.; Wagner, H.J.; Bartsch, D.K. Successful treatment of solid-pseudopapillary tumor of the pancreas with multiple liver metastases. Pancreatology 2005, 5, 289–294. [Google Scholar] [CrossRef]
- Zhan, H.; Cheng, Y.; Wang, L.; Su, P.; Zhong, N.; Zhang, Z. Clinicopathological Features and Treatment Outcomes of Solid Pseudopapillary Neoplasms of the Pancreas: A 10-Year Case Series from a Single Center. J. Laparoendosc. Adv. Surg. Tech. 2019, 29, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, V.; Pozza, G.; Dalla Bona, E.; Fantin, A.; Valmasoni, M.; Sperti, C. Solid-Pseudopapillary Tumor of the Pancreas: A Single Center Experience. Gastroenterol. Res. Pract. 2016, 2016, 4289736. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.J.; Javed, A.A.; Saunders, T.; Zhu, Y.; Burkhart, R.A.; Yu, J. Surgical Resection of 78 Pancreatic Solid Pseudopapillary Tumors: A 30-Year Single Institutional Experience. J. Gastrointest. Surg. 2020, 24, 874–881. [Google Scholar] [CrossRef]
- Ventriglia, A.; Manfredi, R.; Mehrabi, S.; Boninsegna, E.; Negrelli, R.; Pedrinolla, B.; Pozzi Mucelli, R. MRI features of solid pseudopapillary neoplasm of the pancreas. Abdom. Imaging 2014, 39, 1213–1220. [Google Scholar] [CrossRef]
- Chae, S.H.; Lee, J.M.; Baek, J.H.; Shin, C.I.; Yoo, M.H.; Yoon, J.H.; Kim, J.H.; Han, J.K.; Choi, B.I. Magnetic resonance imaging spectrum of solid pseudopapillary neoplasm of the pancreas. J. Comput. Assist. Tomogr. 2014, 38, 249–257. [Google Scholar] [CrossRef]
- Guerrache, Y.; Soyer, P.; Dohan, A.; Faraoun, S.A.; Laurent, V.; Tasu, J.P.; Aubé, C.; Cazejust, J.; Boudiaf, M.; Hoeffel, C. Solid-pseudopapillary tumor of the pancreas: MR imaging findings in 21 patients. Clin. Imaging 2014, 38, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Coleman, K.M.; Doherty, M.C.; Bigler, S.A. Solid-pseudopapillary tumor of the pancreas. Radiographics 2003, 23, 1644–1648. [Google Scholar] [CrossRef]
- Baek, J.H.; Lee, J.M.; Kim, S.H.; Kim, S.J.; Kim, S.H.; Lee, J.Y.; Han, J.K.; Choi, B.I. Small (≤3 cm) Solid Pseudopapillary Tumors of the Pancreas at Multiphasic Multidetector CT 1. Radiology 2010, 257, 97–106. [Google Scholar] [CrossRef]
- Liu, M.; Liu, J.; Hu, Q.; Xu, W.; Liu, W.; Zhang, Z.; Sun, Q.; Qin, Y.; Yu, X.; Ji, S.; et al. Management of solid pseudopapillary neoplasms of pancreas: A single center experience of 243 consecutive patients. Pancreatology 2019, 19, 681–685. [Google Scholar] [CrossRef]
- Morito, A.; Eto, K.; Matsuishi, K.; Hamasaki, H.; Morita, K.; Ikeshima, S.; Horino, K.; Shimada, S.; Baba, H. A case of repeat hepatectomy for liver mastasis from solid pseudopapillary neoplasm of the pancreas: A case report. Surg. Case Rep. 2021, 7, 60. [Google Scholar] [CrossRef]
- Law, J.K.; Ahmed, A.; Singh, V.K.; Akshintala, V.S.; Olson, M.T.; Raman, S.P.; Ali, S.Z.; Fishman, E.K.; Kamel, I.; Canto, M.I.; et al. A systematic review of solid-pseudopapillary neoplasms: Are these rare lesions? Pancreas 2014, 43, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Jin, C.; Long, J.; Yu, X.J.; Xu, J.; Di, Y.; Li, J.; de Fu, L.; Ni, Q.X. Solid pseudopapillary tumor of the pancreas: A case series of 26 consecutive patients. Am. J. Surg. 2009, 198, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Devi, J.; Sathyalakshmi, R.; Chandramouleeswari, K.; Devi, N.R. Pancreatic schwannoma—A rare case report. J. Clin. Diagn. Res. 2014, 8, FD15–FD16. [Google Scholar]
- Antinheimo, J.; Sankila, R.; Carpén, O.; Pukkala, E.; Sainio, M.; Jääskeläinen, J. Population-based analysis of sporadic and type 2 neurofibromatosis-associated meningiomas and schwannomas. Neurology 2000, 54, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Siegelman, E.S.; Lee, M.K., 4th; Tondon, R. Pancreatic schwannoma, an extremely rare and challenging entity: Report of two cases and review of literature. Pancreatology 2019, 19, 729–737. [Google Scholar] [CrossRef]
- Varshney, V.K.; Yadav, T.; Elhence, P.; Sureka, B. Preoperative diagnosis of pancreatic schwannoma—Myth or reality. J. Cancer Res. Ther. 2020, 16, S222–S226. [Google Scholar] [CrossRef]
- Kinhal, V.A.; Ravishankar, T.H.; Melapure, A.I.; Jayaprakasha, G.; Range Gowda, B.C.; Manjunath. Pancreatic schwannoma: Report of a case and review of literature. Indian J. Surg. 2010, 72, 296–298. [Google Scholar] [CrossRef]
- Ma, Y.; Shen, B.; Jia, Y.; Luo, Y.; Tian, Y.; Dong, Z.; Chen, W.; Li, Z.P.; Feng, S.T. Pancreatic schwannoma: A case report and an updated 40-year review of the literature yielding 68 cases. BMC Cancer 2017, 14, 853. [Google Scholar]
- Wang, H.; Zhang, B.B.; Wang, S.F.; Zhong, J.J.; Zheng, J.M.; Han, H. Pancreatic schwannoma: Imaging features and pathological findings. Hepatobiliary Pancreat. Dis. Int. HBPD INT 2020, 19, 200–202. [Google Scholar] [CrossRef]
- Tofigh, A.M.; Hashemi, M.; Honar, B.N.; Solhjoo, F. Rare presentation of pancreatic schwannoma: A case report. J. Med. Case Rep. 2008, 12, 268. [Google Scholar] [CrossRef]
- Abu-Zaid, A.; Azzam, A.; Abou Al-Shaar, H.; Alshammari, A.M.; Amin, T.; Mohammed, S. Pancreatic tail schwannoma in a 44-year-old male: A case report and literature review. Case Rep. Oncol. Med. 2013, 2013, 416713. [Google Scholar] [CrossRef] [PubMed]
- Moriya, T.; Kimura, W.; Hirai, I.; Takeshita, A.; Tezuka, K.; Watanabe, T.; Mizutani, M.; Fuse, A. Pancreatic schwannoma: Case report and an updated 30-year review of the literature yielding 47 cases. World J. Gastroenterol. 2012, 18, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Novellas, S.; Chevallier, P.; Saint Paul, M.C.; Gugenheim, J.; Bruneton, J.N. MRI features of a pancreatic schwannoma. Clin. Imaging 2005, 29, 434–436. [Google Scholar] [CrossRef]
- Yu, R.S.; Sun, J.Z. Pancreatic schwannoma: CT findings. Abdom. Imaging 2006, 31, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Hamada, K.; Ueda, T.; Higuchi, I.; Inoue, A.; Tamai, N.; Myoi, A.; Tomita, Y.; Aozasa, K.; Yoshikawa, H.; Hatazawa, J. Peripheral nerve schwannoma: Two cases exhibiting increased FDG uptake in early and delayed PET imaging. Skelet. Radiol. 2005, 34, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Birk, H.; Zygourakis, C.C.; Kliot, M. Developing an algorithm for cost-effective, clinically judicious management of peripheral nerve tumors. Surg. Neurol. Int. 2016, 7, 80. [Google Scholar]
- Wang, S.; Xing, C.; Wu, H.; Dai, M.; Zhao, Y. Pancreatic schwannoma mimicking pancreatic cystadenoma: A case report and literature review of the imaging features. Medicine 2019, 98, e16095. [Google Scholar] [CrossRef]
- Shimizu, K.; Shiratori, K.; Toki, F.; Suzuki, M.; Imaizumi, T.; Takasaki, K.; Kobayashi, M.; Hayashi, N. Nonfunctioning islet cell tumor with a unique pattern of tumor growth. Dig. Dis. Sci. 1999, 44, 547–551. [Google Scholar] [CrossRef]
- Akatsu, T.; Wakabayashi, G.; Aiura, K.; Suganuma, K.; Takigawa, Y.; Wada, M.; Kawachi, S.; Tanabe, M.; Ueda, M.; Shimazu, M.; et al. Intraductal growth of a nonfunctioning endocrine tumor of the pancreas. J. Gastroenterol. 2004, 39, 584–588. [Google Scholar] [CrossRef]
- Fassan, M.; Pizzi, S.; Pasquali, C.; Parenti, A.R. Pancreatic endocrine tumor in multiple endocrine neoplasia type 1syndrome with intraductal growth into the main pancreatic duct. Pancreas 2009, 38, 341–342. [Google Scholar] [CrossRef]
- Inagaki, M.; Watanabe, K.; Yoshikawa, D.; Suzuki, S.; Ishizaki, A.; Matsumoto, K.; Haneda, M.; Tokusashi, Y.; Miyokawa, N.; Sato, S.; et al. A malignant nonfunctioning pancreatic endocrine tumor with unique pattern of intraductal growth. J. Hepatobiliary Pancreat. Surg. 2007, 14, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, H.; Kuwatani, M.; Hirano, S.; Kondo, S.; Nakanishi, Y.; Itoh, T.; Asaka, M. Pancreatic endocrine tumors with intraductal growth into the main pancreatic duct and tumor thrombus within the portal vein: A case report and review of the literature. Int. Med. 2007, 46, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Kitami, C.E.; Shimizu, T.; Sato, O.; Kurosaki, I.; Mori, S.; Yanagisawa, Y.; Ajioka, Y.; Hatakeyama, K. Malignant islet cell tumor projecting into the main pancreatic duct. J. Hepatobiliary Pancreat. Surg. 2000, 7, 529–533. [Google Scholar] [CrossRef]
- Terada, T.; Kawaguchi, M.; Furukawa, K.; Sekido, Y.; Osamura, Y. Minute mixed ductal-endocrine carcinoma of the pancreas with predominant intraductal growth. Pathol. Int. 2002, 52, 740–746. [Google Scholar] [CrossRef]
- D’Onofrio, M.; Capelli, P.; Pederzoli, P. Imaging and Pathology of Pancreatic Neoplasms. A Pictorial Atlas, 1st ed.; Springer Science + Business Media: Milan, Italy, 2015. [Google Scholar]
- Yazawa, N.; Imaizumi, T.; Okada, K.; Matsuyama, M.; Dowaki, S.; Tobita, K.; Ohtani, Y.; Ogoshi, K.; Hirabayashi, K.; Makuuchi, H. Nonfunctioning pancreatic endocrine tumor with extension into the main pancreatic duct: Report of a case. Surg. Today 2011, 41, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Chetty, R.; El-Shinnawy, I. Intraductal pancreatic neuroendocrine tumor. Endocr. Pathol. 2009, 20, 262–266. [Google Scholar] [CrossRef]
- Ciaravino, V.; De Robertis, R.; Tinazzi Martini, P.; Cardobi, N.; Cingarlini, S.; Amodio, A.; Landoni, L.; Capelli, P.; D’Onofrio, M. Imaging presentation of pancreatic neuroendocrine neoplasms. Insights Imaging 2018, 9, 943–953. [Google Scholar] [CrossRef]
- Klemperer, P.; Coleman, B.R. Primary neoplasms of the pleura. A report of five cases. Am. J. Ind. Med. 1992, 22, 4–31. [Google Scholar] [CrossRef]
- Manning, M.A.; Paal, E.E.; Srivastava, A.; Mortele, K.J. Nonepithelial Neoplasms of the Pancreas, Part 2: Malignant Tumors and Tumors of Uncertain Malignant Potential From the Radiologic Pathology Archives. Radiographics 2018, 38, 1047–1072. [Google Scholar] [CrossRef]
- Taguchi, Y.; Hara, T.; Tamura, H.; Ogiku, M.; Watahiki, M.; Takagi, T.; Harada, T.; Miyazaki, S.; Hayashi, T.; Kanai, T.; et al. Malignant solitary fibrous tumor of the pancreas: A case report. Surg. Case Rep. 2020, 136, 287. [Google Scholar] [CrossRef]
- Li, J.; Li, J.; Xiong, Y.; Xu, T.; Xu, J.; Li, Q.; Yang, G. Atypical/malignant solitary fibrous tumor of the pancreas with spleen vein invasion: Case report and literature review. Medicine 2020, 99, e19783. [Google Scholar] [CrossRef] [PubMed]
- Fung, E.C.; Crook, M.A. Doege-Potter syndrome and ‘big-IGF2’: A rare cause of hypoglycaemia. Ann. Clin. Biochem. 2011, 48 Pt 2, 95–96. [Google Scholar] [CrossRef] [PubMed]
- Shanbhogue, A.K.; Prasad, S.R.; Takahashi, N.; Vikram, R.; Zaheer, A.; Sandrasegaran, K. Somatic and visceral solitary fibrous tumors in the abdomen and pelvis: Cross-sectional imaging spectrum. Radiographics 2011, 31, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.C.; Huang, H.Y. Solitary fibrous tumor: An evolving and unifying entity with unsettled issues. Histol. Histopathol. 2019, 34, 313–334. [Google Scholar]
- Ginat, D.T.; Bokhari, A.; Bhatt, S.; Dogra, V. Imaging features of solitary fibrous tumors. AJR Am. J. Roentgenol. 2011, 196, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Martin-Broto, J.; Mondaza-Hernandez, J.L.; Moura, D.S.; Hindi, N. A Comprehensive Review on Solitary Fibrous Tumor: New Insights for New Horizons. Cancers 2021, 13, 2913. [Google Scholar] [CrossRef]
- Srinivasan, V.D.; Wayne, J.D.; Rao, M.S.; Zynger, D.L. Solitary fibrous tumor of the pancreas: Case report with cytologic and surgical pathology correlation and review of the literature. J. Pancreas 2008, 9, 526–530. [Google Scholar]
- Davanzo, B.; Emerson, R.E.; Lisy, M.; Koniaris, L.G.; Kays, J.K. Solitary fibrous tumor. Transl. Gastroenterol. Hepatol. 2018, 3, 94. [Google Scholar] [CrossRef]
- Kayani, B.; Sharma, A.; Sewell, M.D.; Platinum, J.; Olivier, A.; Briggs, T.W.R.; Eastwood, D.M. A Review of the Surgical Management of Extrathoracic Solitary Fibrous Tumors. Am. J. Clin. Oncol. 2018, 41, 687–694. [Google Scholar] [CrossRef]
- Robinson, L.A. Solitary fibrous tumor of the pleura. Cancer Control 2006, 13, 264–269. [Google Scholar] [CrossRef]
- Ordóñez, N.G. Pancreatic acinar cell carcinoma. Adv. Anat. Pathol. 2001, 8, 144–159. [Google Scholar] [PubMed]
- Toll, A.D.; Hruban, R.H.; Ali, S.Z. Acinar cell carcinoma of the pancreas: Clinical and cytomorphologic characteristics. Korean J. Pathol. 2013, 47, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, P. Acinar Cell Carcinoma of the Pancreas: A Literature Review and Update. Indian J. Surg. 2015, 77, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Lack, E.E.; Cassady, J.R.; Levey, R.; Vawter, G.F. Tumors of the exocrine pancreas in children and adolescents. A clinical and pathologic study of eight cases. Am. J. Surg. Pathol. 1983, 7, 319–327. [Google Scholar] [CrossRef]
- Bhosale, P.; Balachandran, A.; Wang, H.; Wei, W.; Hwang, R.F.; Fleming, J.B.; Varadhachary, G.; Charnsangavej, C.; Tamm, E. CT imaging features of acinar cell carcinoma and its hepatic metastases. Abdom. Imaging 2013, 38, 1383–1390. [Google Scholar] [CrossRef]
- Klimstra, D.S.; Heffess, C.S.; Oertel, J.E.; Rosai, J. Acinar cell carcinoma of the pancreas. A clinicopathologic study of 28 cases. Am. J. Surg. Pathol. 1992, 16, 815–837. [Google Scholar] [CrossRef]
- Hsu, M.Y.; Pan, K.T.; Chu, S.Y.; Hung, C.F.; Wu, R.C.; Tseng, J.H. CT and MRI features of acinar cell carcinoma of the pancreas with pathological correlations. Clin. Radiol. 2010, 65, 223–229. [Google Scholar] [CrossRef]
- Fabre, A.; Sauvanet, A.; Flejou, J.F.; Belghiti, J.; Palazzo, L.; Ruszniewski, P.; Degott, C.; Terris, B. Intraductal acinar cell carcinoma of the pancreas. Virchows Arch. 2001, 438, 312–315. [Google Scholar] [CrossRef]
- Calimano-Ramirez, L.F.; Daoud, T.; Gopireddy, D.R.; Morani, A.C.; Waters, R.; Gumus, K.; Klekers, A.R.; Bhosale, P.R.; Virarkar, M.K. Pancreatic acinar cell carcinoma: A comprehensive review. World J. Gastroenterol. 2022, 28, 5827–5844. [Google Scholar] [CrossRef]
- Borowicz, J.; Morrison, M.; Hogan, D.; Miller, R. Subcutaneous fat necrosis/panniculitis and polyarthritis associated with acinar cell carcinoma of the pancreas: A rare presentation of pancreatitis, panniculitis and polyarthritis syndrome. J. Drugs Dermatol. 2010, 9, 1145–1150. [Google Scholar]
- Radin, D.R.; Colletti, P.M.; Forrester, D.M.; Tang, W.W. Pancreatic acinar cell carcinoma with subcutaneous and intraosseous fat necrosis. Radiology 1986, 158, 67–68. [Google Scholar] [CrossRef] [PubMed]
- Burns, W.A.; Matthews, M.J.; Hamosh, M.; Weide, G.V.; Blum, R.; Johnson, F.B. Lipase-secreting acinar cell carcinoma of the pancreas with polyarthropathy. A light and electron microscopic, histochemical, and biochemical study. Cancer 1974, 33, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Cingolani, N.; Shaco-Levy, R.; Farruggio, A.; Klimstra, D.S.; Rosai, J. Alpha-fetoprotein production by pancreatic tumors exhibiting acinar cell differentiation: Study of five cases, one arising in a mediastinal teratoma. Hum. Pathol. 2000, 31, 938–944. [Google Scholar] [CrossRef] [PubMed]
- Raman, S.P.; Hruban, R.H.; Cameron, J.L.; Wolfgang, C.L.; Fishman, E.K. Pancreatic imaging mimics: Part 2, pancreatic neuroendocrine tumors and their mimics. AJR Am. J. Roentgenol. 2012, 199, 309–318. [Google Scholar] [CrossRef]
- Raman, S.P.; Hruban, R.H.; Cameron, J.L.; Wolfgang, C.L.; Kawamoto, S.; Fishman, E.K. Acinar cell carcinoma of the pancreas: Computed tomography features—A study of 15 patients. Abdom. Imaging 2013, 38, 137–143. [Google Scholar] [CrossRef]
- Chiou, Y.Y.; Chiang, J.H.; Hwang, J.I.; Yen, C.H.; Tsay, S.H.; Chang, C.Y. Acinar cell carcinoma of the pancreas: Clinical and computed tomography manifestations. J. Comput. Assist. Tomogr. 2004, 28, 180–186. [Google Scholar] [CrossRef]
- Thompson, E.D.; Wood, L.D. Pancreatic Neoplasms With Acinar Differentiation: A Review of Pathologic and Molecular Features. Arch. Pathol. Lab. Med. 2020, 144, 808–815. [Google Scholar] [CrossRef]
- Tatli, S.; Mortele, K.J.; Levy, A.D.; Glickman, J.N.; Ros, P.R.; Banks, P.A.; Silverman, S.G. CT and MRI features of pure acinar cell carcinoma of the pancreas in adults. AJR Am. J. Roentgenol. 2005, 184, 511–519. [Google Scholar] [CrossRef]
- Javadi, S.; Menias, C.O.; Korivi, B.R.; Shaaban, A.M.; Patnana, M.; Alhalabi, K.; Elsayes, K.M. Pancreatic Calcifications and Calcified Pancreatic Masses: Pattern Recognition Approach on CT. Am. J. Roentgenol. 2017, 209, 77–87. [Google Scholar] [CrossRef]
- Klöppel, G.; Kosmahl, M. Cystic lesions and neoplasms of the pancreas. The features are becoming clearer. Pancreatology 2001, 1, 648–655. [Google Scholar] [CrossRef]
- Mergo, P.J.; Helmberger, T.K.; Buetow, P.C.; Helmberger, R.C.; Ros, P.R. Pancreatic neoplasms: MR imaging and pathologic correlation. Radiographics 1997, 17, 281–301. [Google Scholar] [CrossRef] [PubMed]
- Cantisani, V.; Mortele, K.J.; Levy, A.; Glickman, J.N.; Ricci, P.; Passariello, R.; Ros, P.R.; Silverman, S.G. MR imaging features of solid pseudopapillary tumor of the pancreas in adult and pediatric patients. Am. J. Roentgenol. 2003, 181, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Solcia, E.; Capella, C.; Kloppel, G. Tumors of the exocrine pancreas. In Atlas of Tumor Pathology: Tumors of the Pancreas; Rosai, J., Sorbin, L., Eds.; Armed Forces Institute of Pathology: Washington, DC, USA, 1997; pp. 31–144. [Google Scholar]
- Distler, M.; Rückert, F.; Dittert, D.D.; Stroszczynski, C.; Dobrowolski, F.; Kersting, S.; Grützmann, R. Curative resection of a primarily unresectable acinar cell carcinoma of the pancreas after chemotherapy. World J. Surg. Oncol. 2009, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Mortenson, M.M.; Katz, M.H.; Tamm, E.P.; Bhutani, M.S.; Wang, H.; Evans, D.B.; Fleming, J.B. Current diagnosis and management of unusual pancreatic tumors. Am. J. Surg. 2008, 196, 100–113. [Google Scholar] [CrossRef]
- Matos, J.M.; Schmidt, C.M.; Turrini, O.; Agaram, N.P.; Niedergethmann, M.; Saeger, H.D.; Merchant, N.; Johnson, C.S.; Lillemoe, K.D.; Grützmann, R. Pancreatic acinar cell carcinoma: A multi-institutional study. J. Gastrointest. Surg. 2009, 13, 1495–1502. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, S.; Zhou, X.; Zhou, H.; Cui, Y.; Li, Q.; Zhang, L. Acinar cell carcinoma: A report of 19 cases with a brief review of the literature. World J. Surg. Oncol. 2016, 14, 172. [Google Scholar] [CrossRef]
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- Muraki, T.; Reid, M.D.; Basturk, O.; Jang, K.T.; Bedolla, G.; Bagci, P.; Mittal, P.; Memis, B.; Katabi, N.; Bandyopadhyay, S.; et al. Undifferentiated Carcinoma With Osteoclastic Giant Cells of the Pancreas: Clinicopathologic Analysis of 38 Cases Highlights a More Protracted Clinical Course Than Currently Appreciated. Am. J. Surg. Pathol. 2016, 40, 1203–1216. [Google Scholar] [CrossRef]
- Jo, S. Huge undifferentiated carcinoma of the pancreas with osteoclast-like giant cells. World J. Gastroenterol. 2014, 20, 2725–2730. [Google Scholar] [CrossRef]
- Kalluri, R.; Weinberg, R.A. The basics of epithelial-mesenchymal transition. J. Clin. Investig. 2010, 119, 1420–1428. [Google Scholar] [CrossRef]
- Nieto, M.A.; Huang, R.Y.; Jackson, R.A.; Thiery, J.P. EMT: 2016. Cell 2016, 166, 21–45. [Google Scholar] [CrossRef] [PubMed]
- Lambert, A.W.; Pattabiraman, D.R.; Weinberg, R.A. Emerging Biological Principles of Metastasis. Cell 2017, 168, 670–691. [Google Scholar] [CrossRef] [PubMed]
- Joo, Y.E.; Heo, T.; Park, C.H.; Lee, W.S.; Kim, H.S.; Kim, J.C.; Koh, Y.S.; Choi, S.K.; Cho, C.K.; Rew, J.S.; et al. A case of osteoclast-like giant cell tumor of the pancreas with ductal adenocarcinoma: Histopathological, immunohistochemical, ultrastructural and molecular biological studies. J. Korean Med. Sci. 2005, 20, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, E.; Schena, N.; Serino, G.; Lantone, G.; Armentano, R. Assessment and management of undifferentiated carcinoma with osteoclastic like giant cells of the pancreas: A case report and revision of literature. BMC Gastroenterol. 2021, 21, 247. [Google Scholar] [CrossRef]
- Yang, K.Y.; Choi, J.I.; Choi, M.H.; Park, M.Y.; Rha, S.E.; Byun, J.Y.; Jung, E.S.; Lall, C. Magnetic resonance imaging findings of undifferentiated carcinoma with osteoclast-like giant cells of pancreas. Clin. Imaging 2016, 40, 148–151. [Google Scholar] [CrossRef]
- Maksymov, V.; Khalifa, M.A.; Bussey, A.; Carter, B.; Hogan, M. Undifferentiated (anaplastic) carcinoma of the pancreas with osteoclast-like giant cells showing various degree of pancreas duct involvement. A case report and literature review. JOP 2011, 12, 170–176. [Google Scholar]
- Yazawa, T.; Watanabe, A.; Araki, K.; Segawa, A.; Hirai, K.; Kubo, N.; Igarashi, T.; Tsukagoshi, M.; Ishii, N.; Hoshino, K.; et al. Complete resection of a huge pancreatic undifferentiated carcinoma with osteoclast-like giant cells. Int. Cancer Conf. J. 2017, 6, 193–196. [Google Scholar] [CrossRef]
- Gao, H.Q.; Yang, Y.M.; Zhuang, Y.; Liu, P. Locally advanced undifferentiated carcinoma with osteoclast-like giant cells of the pancreas. World J. Gastroenterol. 2015, 21, 694–698. [Google Scholar] [CrossRef]
- Sakhi, R.; Hamza, A.; Khurram, M.S.; Ibrar, W.; Mazzara, P. Undifferentiated carcinoma of the pancreas with osteoclast-like giant cells reported in an asymptomatic patient: A rare case and literature review. Autops. Case Rep. 2017, 7, 51–57. [Google Scholar] [CrossRef]
- Togawa, Y.; Tonouchi, A.; Chiku, T.; Sano, W.; Doki, T.; Yano, K.; Uno, H.; Muronoi, T.; Kaneoya, K.; Shinagawa, T.; et al. A case report of undifferentiated carcinoma with osteoclast-like giant cells of the pancreas and literature review. Clin. J. Gastroenterol. 2010, 3, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, T.; Federle, M.P.; Ohba, S.; Ohtomo, K.; Sugiyama, A.; Fujimoto, H.; Haradome, H.; Araki, T. Atypical exocrine and endocrine pancreatic tumors (anaplastic, small cell, and giant cell types): CT and pathologic features in 14 patients. Abdom. Imaging 2000, 25, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Itano, O.; Oshima, G.; Chiba, N.; Ishikawa, H.; Koyama, Y.; Du, W.; Kitagawa, Y. A male case of an undifferentiated carcinoma with osteoclast-like giant cells originating in an indeterminate mucin-producing cystic neoplasm of the pancreas. A case report and review of the literature. World J. Surg. Oncol. 2011, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Urakawa, H.; Sakamoto, K.; Ito, E.; Hamada, Y.; Yoshimitsu, K. Undifferentiated carcinoma of the pancreas with osteoclast-like giant cells showing intraductal growth and intratumoral hemorrhage: MRI features. Radiol. Case Rep. 2019, 14, 1283–1287. [Google Scholar] [CrossRef] [PubMed]
- Oehler, U.; Jurs, M.; Kloppel, G.; Helpap, B. Osteoclast-like giant cell tumour of the pancreas presenting as a pseudocyst-like lesion. Virchows Arch. 1997, 431, 215–218. [Google Scholar] [CrossRef]
- Molberg, K.H.; Heffess, C.; Delgado, R.; Albores-Saavedra, J. Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas and periampullary region. Cancer 1998, 82, 1279–1287. [Google Scholar] [CrossRef]
- Zou, X.P.; Yu, Z.L.; Li, Z.S.; Zhou, G.Z. Clinicopathological features of giant cell carcinoma of the pancreas. Hepatobiliary Pancreat. Dis. Int. 2004, 3, 300–302. [Google Scholar]
- Paal, E.; Thompson, L.D.; Frommelt, R.A.; Przygodzki, R.M.; Heffess, C.S. A clinicopathologic and immunohistochemical study of 35 anaplastic carcinomas of the pancreas with a review of the literature. Ann. Diagn. Pathol. 2001, 5, 129–140. [Google Scholar] [CrossRef]
- Hirano, H.; Morita, K.; Tachibana, S.; Okimura, A.; Fujisawa, T.; Ouchi, S.; Nakasho, K.; Ueyama, S.; Nishigami, T.; Terada, N. Undifferentiated carcinoma with osteoclast-like giant cells arising in a mucinous cystic neoplasm of the pancreas. Pathol. Int. 2008, 58, 383–389. [Google Scholar] [CrossRef]
- Demetter, P.; Maréchal, R.; Puleo, F.; Delhaye, M.; Debroux, S.; Charara, F.; Gomez Galdon, M.; Van Laethem, J.L.; Verset, L. Undifferentiated Pancreatic Carcinoma with Osteoclast-like Giant Cells: What Do We Know So Far? Front. Oncol. 2021, 11, 630086. [Google Scholar] [CrossRef]
- Luchini, C.; Pea, A.; Lionheart, G.; Mafficini, A.; Nottegar, A.; Veronese, N.; Chianchiano, P.; Brosens, L.A.; Noë, M.; Offerhaus, G.J.A.; et al. Pancreatic undifferentiated carcinoma with osteoclast-like giant cells is genetically similar to, but clinically distinct from, conventional ductal adenocarcinoma. J. Pathol. 2017, 243, 148–154. [Google Scholar] [CrossRef]
- Moore, J.C.; Bentz, J.S.; Hilden, K.; Adler, D.G. Osteoclastic and pleomorphic giant cell tumors of the pancreas: A review of clinical, endoscopic, and pathologic features. World J. Gastrointest. Endosc. 2010, 2, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Boyd, C.A.; Benarroch-Gampel, J.; Sheffield, K.M.; Cooksley, C.D.; Riall, T.S. 415 patients with adenosquamous carcinoma of the pancreas: A population-based analysis of prognosis and survival. J. Surg. Res. 2012, 174, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Borazanci, E.; Millis, S.Z.; Korn, R.; Han, H.; Whatcott, C.J.; Gatalica, Z.; Barrett, M.T.; Cridebring, D.; Von Hoff, D.D. Adenosquamous carcinoma of the pancreas: Molecular characterization of 23 patients along with a literature review. World J. Gastrointest. Oncol. 2015, 7, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Simone, C.G.; Zuluaga Toro, T.; Chan, E.; Feely, M.M.; Trevino, J.G.; George, T.J., Jr. Characteristics and outcomes of adenosquamous carcinoma of the pancreas. Gastrointest. Cancer Res. 2013, 6, 75–79. [Google Scholar] [CrossRef]
- Herxheimer, G. Über heterologe Cancroide. Beitr. Pathol. Anat. 1907, 41, 348–412. [Google Scholar]
- Hruban, R.H.; Pitman, M.B.; Klimstra, D.S. Tumors of the Pancreas, Afip Atlas of Tumor Pathology, 4th Series Fascicle 6, 6th ed.; American Registry of Pathology: Washington, DC, USA, 2007. [Google Scholar]
- Voong, K.R.; Davison, J.; Pawlik, T.M.; Uy, M.O.; Hsu, C.C.; Winter, J.; Hruban, R.H.; Laheru, D.; Rudra, S.; Swartz, M.J.; et al. Resected pancreatic adenosquamous carcinoma: Clinicopathologic review and evaluation of adjuvant chemotherapy and radiation in 38 patients. Hum. Pathol. 2010, 41, 113–122. [Google Scholar] [CrossRef]
- Kardon, D.E.; Thompson, L.D.; Przygodzki, R.M.; Heffess, C.S. Adenosquamous carcinoma of the pancreas: A clinicopathologic series of 25 cases. Mod. Pathol. 2001, 14, 443–451. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Enjoji, M. Adenosquamous carcinoma of the pancreas: A clinicopathologic study. J. Surg. Oncol. 1991, 47, 109–116. [Google Scholar] [CrossRef]
- Murakami, Y.; Yokoyama, T.; Yokoyama, Y.; Kanehiro, T.; Uemura, K.; Sasaki, M.; Morifuji, M.; Sueda, T. Adenosquamous carcinoma of the pancreas: Preoperative diagnosis and molecular alterations. J. Gastroenterol. 2003, 38, 1171–1175. [Google Scholar] [CrossRef]
- Trikudanathan, G.; Dasanu, C.A. Adenosquamous carcinoma of the pancreas: A distinct clinicopathologic entity. South. Med. J. 2010, 103, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Momosaki, S.; Yano, H.; Kojiro, M. Establishment of a human hepatic adenosquamous carcinoma cell line (KMC-2) and its response to cytokines. Pathol. Int. 1995, 45, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Madura, J.A.; Jarman, B.T.; Doherty, M.G.; Yum, M.N.; Howard, T.J. Adenosquamous carcinoma of the pancreas. Arch. Surg. 1999, 134, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Kovi, J. Adenosquamous carcinoma of the pancreas: A light and electron microscopic study. Ultrastruct. Pathol. 1982, 3, 17–23. [Google Scholar] [CrossRef]
- Xiong, Q.; Zhang, Z.; Xu, Y.; Zhu, Q. Pancreatic Adenosquamous Carcinoma: A Rare Pathological Subtype of Pancreatic Cancer. J. Clin. Med. 2022, 11, 7401. [Google Scholar] [CrossRef]
- Yin, Q.; Wang, C.; Wu, Z.; Wang, M.; Cheng, K.; Zhao, X.; Yuan, F.; Tang, Y.; Miao, F. Adenosquamous carcinoma of the pancreas: Multidetector-row computed tomographic manifestations and tumor characteristics. J. Comput. Assist. Tomogr. 2013, 37, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Nagao, S.; Tajima, H.; Okudaira, K.; Hashiguchi, K.; Miyazaki, J.; Matsuzaki, K.; Tsuzuki, Y.; Kawaguchi, A.; Itoh, K.; et al. Adenosquamous pancreatic cancer producing parathyroid hormone-related protein. J. Gastroenterol. 2004, 39, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Higurashi, T.; Iida, H.; Mawatari, H.; Endo, H.; Nozaki, Y.; Tomimoto, A.; Yoneda, K.; Akiyama, T.; Fujita, K.; et al. Adenosquamous carcinoma of the pancreas associated with humoral hypercalcemia of malignancy (HHM). J. Hepatobiliary Pancreat. Surg. 2008, 15, 531–535. [Google Scholar] [CrossRef]
- López-Tomassetti-Fernández, E.M.; Favre-Rizzo, J.; Delgado-Plasencia, L.; Hernández-Hernández, J.R. Hypercalcemia associated with adenosquamous pancreatic carcinoma: A reason to initiate palliative treatment. Rev. Esp. Enferm. Dig. 2013, 105, 425–428. [Google Scholar] [CrossRef]
- Hsu, J.T.; Chen, H.M.; Wu, R.C.; Yeh, C.N.; Yeh, T.S.; Hwang, T.L.; Jan, Y.Y.; Chen, M.F. Clinicopathologic features and outcomes following surgery for pancreatic adenosquamous carcinoma. World J. Surg. Oncol. 2008, 6, 95. [Google Scholar] [CrossRef]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goéré, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. ESMO Guidelines Committee. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26 (Suppl. 5), v56–v68. [Google Scholar] [CrossRef] [PubMed]
- Wahab, A.; Gonzalez, J.J.; Devarkonda, V.; Saint-Phard, T.; Singh, T.; Adekolujo, O.S. Squamous cell carcinoma-A rare pancreatic exocrine malignancy. Cancer Biol. Ther. 2019, 20, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Itani, K.M.; Karni, A.; Green, L. Squamous cell carcinoma of the pancreas. J. Gastrointest. Surg. 1999, 3, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Horino, K.; Takamori, H.; Ikuta, Y.; Nakahara, O.; Chikamoto, A.; Ishiko, T.; Beppu, T.; Baba, H. Cutaneous metastases secondary to pancreatic cancer. World J. Gastrointest. Oncol. 2012, 4, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.Y.; Wang, X.B.; Gao, F.; Bu, B.; Zhang, S.; Wang, Z. Cutaneous metastasis from pancreatic cancer: A case report and systematic review of the literature. Oncol. Lett. 2014, 8, 2654–2660. [Google Scholar] [CrossRef]
- Miyahara, M.; Hamanaka, Y.; Kawabata, A.; Sato, Y.; Tanaka, A.; Yamamoto, A.; Ueno, T.; Nishihara, K.; Suzuki, T. Cutaneous metastases from pancreatic cancer. Int. J. Pancreatol. 1996, 20, 127–130. [Google Scholar] [CrossRef]
- Ding, Y.; Zhou, J.; Sun, H.; He, D.; Zeng, M.; Rao, S. Contrast-enhanced multiphasic CT and MRI findings of adenosquamous carcinoma of the pancreas. Clin. Imaging 2013, 37, 1054–1060. [Google Scholar] [CrossRef]
- Toshima, F.; Inoue, D.; Yoshida, K.; Yoneda, N.; Minami, T.; Kobayashi, S.; Ikdeda, H.; Matsui, O.; Gabata, T. Adenosquamous carcinoma of pancreas: CT and MR imaging features in eight patients, with pathologic correlations and comparison with adenocarcinoma of pancreas. Abdom. Radiol. 2016, 41, 508–520. [Google Scholar] [CrossRef]
- De Moura, D.T.H.; Coronel, M.; Chacon, D.A.; Tanigawa, R.; Chaves, D.M.; Matuguma, S.E.; Dos Santos, M.E.L.; Jukemura, J.; De Moura, E.G.H. Primary adenosquamous cell carcinoma of the pancreas: The use of endoscopic ultrasound guided—Fine needle aspiration to establish a definitive cytologic diagnosis. Rev. Gastroenterol. Peru 2017, 37, 370–373. [Google Scholar]
- Martínez de Juan, F.; Reolid Escribano, M.; Martínez Lapiedra, C.; Maia de Alcantara, F.; Caballero Soto, M.; Calatrava Fons, A.; Machado, I. Pancreatic adenosquamous carcinoma and intraductal papillary mucinous neoplasm in a CDKN2A germline mutation carrier. World J. Gastrointest. Oncol. 2017, 9, 390–396. [Google Scholar] [CrossRef]
- Paramythiotis, D.; Kyriakidis, F.; Karlafti, E.; Didangelos, T.; Oikonomou, I.M.; Karakatsanis, A.; Poulios, C.; Chamalidou, E.; Vagionas, A.; Michalopoulos, A. Adenosquamous carcinoma of the pancreas: Two case reports and review of the literature. J. Med. Case Rep. 2022, 16, 395. [Google Scholar] [CrossRef] [PubMed]
- Liszka, L.; Zielinska-Pajak, E.; Pajak, J.; Gołka, D. Colloid carcinoma of the pancreas: Review of selected pathological and clinical aspects. Pathology 2008, 40, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Adsay, N.V.; Pierson, C.; Sarkar, F. Colloid (mucinous noncystic) carcinoma of the pancreas. Am. J. Surg. Pathol. 2001, 25, 26–42. [Google Scholar] [CrossRef]
- Aaltonen, L.A.; Hamilton, S.R. Pathology and Genetics of Tumours of the Digestive System; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2000; p. 314. [Google Scholar]
- Waters, J.A.; Schnelldorfer, T.; Aguilar-Saavedra, J.R. Survival after resection for invasive intraductal papillary mucinous neoplasm and for pancreatic adenocarcinoma: A multi-institutional comparison according to American Joint Committee on Cancer Stage. J. Am. Coll. Surg. 2011, 213, 275–283. [Google Scholar] [CrossRef]
- Whang, E.E.; Danial, T.; Dunn, J.C.; Ashley, S.W.; Reber, H.A.; Lewin, T.J.; Tompkins, R.K. The spectrum of mucin-producing adenocarcinoma of the pancreas. Pancreas 2000, 21, 147–151. [Google Scholar] [CrossRef]
- Yoon, M.A.; Lee, J.M.; Kim, S.H.; Lee, J.Y.; Han, J.K.; Choi, B.I.; Choi, J.Y.; Park, S.H.; Lee, M.W. MRI features of pancreatic colloid carcinoma. AJR Am. J. Roentgenol. 2009, 193, W308–W313. [Google Scholar] [CrossRef]
- Nakahashi, G.; Yamaguchi, R.; Watanabe, S. A case of rapid growing mucinous carcinoma of the pancreas without intraductal papillary mucinous neoplasm. J. Biliary Tract. Pancreas 2017, 38, 885–890. [Google Scholar]
- Raut, C.P.; Cleary, K.R.; Staerkel, G.A.; Abbruzzese, J.L.; Wolff, R.A.; Lee, J.H.; Vauthey, J.N.; Lee, J.E.; Pisters, P.W.; Evans, D.B. Intraductal papillary mucinous neoplasms of the pancreas: Effect of invasion and pancreatic margin status on recurrence and survival. Ann. Surg. Oncol. 2006, 13, 582–594. [Google Scholar] [CrossRef]
- Poultsides, G.A.; Reddy, S.; Cameron, J.L.; Hruban, R.H.; Pawlik, T.M.; Ahuja, N.; Jain, A.; Edil, B.H.; Iacobuzio-Donahue, C.A.; Schulick, R.D.; et al. Histopathologic basis for the favorable survival after resection of intraductal papillary mucinous neoplasm-associated invasive adenocarcinoma of the pancreas. Ann. Surg. 2010, 251, 470–476. [Google Scholar] [CrossRef]
- Ren, F.Y.; Shao, C.W.; Zuo, C.J.; Lu, J.P. CT features of colloid carcinomas of the pancreas. Chin. Med. J. 2010, 123, 1329–1332. [Google Scholar]
- Adsay, N.V.; Merati, K.; Nassar, H.; Shia, J.; Sarkar, F.; Pierson, C.R.; Cheng, J.D.; Visscher, D.W.; Hruban, R.H.; Klimstra, D.S. Pathogenesis of colloid (pure mucinous) carcinoma of exocrine organs: Coupling of gel-forming mucin (MUC2) production with altered cell polarity and abnormal cell-stroma interaction may be the key factor in the morphogenesis and indolent behavior of colloid carcinoma in the breast and pancreas. Am. J. Surg. Pathol. 2003, 27, 571–578. [Google Scholar] [PubMed]
- Song, S.J.; Lee, J.M.; Kim, Y.J.; Kim, S.H.; Lee, J.Y.; Han, J.K.; Choi, B.I. Differentiation of intraductal papillary mucinous neoplasms from other pancreatic cystic masses: Comparison of multirow-detector CT and MR imaging using ROC analysis. J. Magn. Reson. Imaging 2007, 26, 86–93. [Google Scholar] [CrossRef]
- Plerhoples, T.A.; Ahdoot, M.; DiMaio, M.A.; Pai, R.K.; Park, W.G.; Poultsides, G.A. Colloid carcinoma of the pancreas. Dig. Dis. Sci. 2011, 56, 1295–1298. [Google Scholar] [CrossRef] [PubMed]
- Flor-de-Lima, B.S.; Freitas, P.; Couto, N.; Castillo-Martin, M.; Santiago, I. Pancreatic intraductal papillary mucinous neoplasm associated colloid carcinoma. Radiol. Case Rep. 2021, 16, 2989–2992. [Google Scholar] [CrossRef]
- Schawkat, K.; Manning, M.A.; Glickman, J.N.; Mortele, K.J. Pancreatic Ductal Adenocarcinoma and Its Variants: Pearls and Perils. Radiographics 2020, 40, 1219–1239. [Google Scholar] [CrossRef] [PubMed]
- Parwani, A.V.; Ali, S.Z. Pathologic quiz case: A 52-year-old woman with jaundice and history of necrotizing pancreatitis. Primary colloid carcinoma of the pancreas. Arch. Pathol. Lab. Med. 2005, 129, 255–256. [Google Scholar] [CrossRef]
- Hirono, S.; Yamaue, H. Surgical strategy for intraductal papillary mucinous neoplasms of the pancreas. Surg. Today 2020, 50, 50–55. [Google Scholar] [CrossRef]
- Marchegiani, G.; Andrianello, S.; Dal Borgo, C.; Secchettin, E.; Melisi, D.; Malleo, G.; Bassi, C.; Salvia, R. Adjuvant chemotherapy is associated with improved postoperative survival in specific subtypes of invasive intraductal papillary mucinous neoplasms (IPMN) of the pancreas: It is time for randomized controlled data. HPB Oxf. 2019, 21, 596–603. [Google Scholar] [CrossRef]
- Sohn, T.A.; Yeo, C.J.; Cameron, J.L.; Koniaris, L.; Kaushal, S.; Abrams, R.A.; Sauter, P.K.; Coleman, J.; Hruban, R.H.; Lillemoe, K.D. Resected adenocarcinoma of the pancreas—616 patients: Results, outcomes, and prognostic indicators. J. Gastrointest. Surg. 2000, 4, 567–579. [Google Scholar] [CrossRef]
- Youngwirth, L.M.; Freischlag, K.; Nussbaum, D.P.; Benrashid, E.; Blazer, D.G. Primary sarcomas of the pancreas: A review of 253 patients from the National Cancer Data Base. Surg. Oncol. 2018, 27, 676–680. [Google Scholar] [CrossRef]
- Baylor, S.M.; Berg, J.W. Cross-classification and survival characteristics of 5,000 cases of cancer of the pancreas. J. Surg. Oncol. 1973, 5, 335–358. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Song, J.S.; Park, H.; Byun, J.H.; Song, K.B.; Kim, K.P.; Kim, S.C.; Hong, S.M. Primary mesenchymal tumors of the pancreas: Single-center experience over 16 years. Pancreas 2014, 43, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Papalampros, A.; Vailas, M.G.; Deladetsima, I.; Moris, D.; Sotiropoulou, M.; Syllaios, A.; Petrou, A.; Felekouras, E. Irreversible electroporation in a case of pancreatic leiomyosarcoma: A novel weapon versus a rare malignancy? World J. Surg. Oncol. 2019, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Søreide, J.A.; Undersrud, E.S.; Al-Saiddi, M.S.; Tholfsen, T.; Søreide, K. Primary Leiomyosarcoma of the Pancreas-a Case Report and a Comprehensive Review. J. Gastrointest. Cancer 2016, 47, 358–365. [Google Scholar] [CrossRef]
- Zalatnai, A.; Kovács, M.; Flautner, L.; Sipos, B.; Sarkady, E.; Bocsi, J. Pancreatic leiomyosarcoma. Case report with immunohistochemical and flow cytometric studies. Virchows Arch. 1998, 432, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Asanuma, Y.; Nanjo, H.; Arakawa, A.; Kusano, T.; Koyama, K.; Shindo, M. A resected case of giant leiomyosarcoma of the pancreas. J. Gastroenterol. 1994, 29, 223–227. [Google Scholar] [CrossRef]
- Muhammad, S.U.; Azam, F.; Zuzana, S. Primary pancreatic leiomyosarcoma: A case report. Cases J. 2008, 1, 280. [Google Scholar] [CrossRef]
- Singla, V.; Arora, A.; Tyagi, P.; Bansal, R.K.; Sharma, P.; Bansal, N.; Kumar, A. Rare cause of recurrent acute pancreatitis due to leiomyosarcoma. Trop. Gastroenterol. 2016, 37, 70–72. [Google Scholar] [CrossRef]
- Xu, J.; Zhang, T.; Wang, T.; You, L.; Zhao, Y. Clinical characteristics and prognosis of primary leiomyosarcoma of the pancreas: A systematic review. World J. Surg. Oncol. 2013, 11, 290. [Google Scholar] [CrossRef]
- Aleshawi, A.J.; Allouh, M.Z.; Heis, F.H.; Tashtush, N.; Heis, H.A. Primary Leiomyosarcoma of the Pancreas: A Comprehensive Analytical Review. J. Gastrointest. Cancer 2020, 51, 433–438. [Google Scholar] [CrossRef]
- Zhang, H.; Jensen, M.H.; Farnell, M.B.; Smyrk, T.C.; Zhang, L. Primary leiomyosarcoma of the pancreas: Study of 9 cases and review of literature. Am. J. Surg. Pathol. 2010, 34, 1849–1856. [Google Scholar] [CrossRef] [PubMed]
- Barral, M.; Faraoun, S.A.; Fishman, E.K.; Dohan, A.; Pozzessere, C.; Berthelin, M.A.; Bazeries, P.; Barat, M.; Hoeffel, C.; Soyer, P. Imaging features of rare pancreatic tumors. Diagn. Interv. Imaging 2016, 97, 1259–1273. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, D.N.; Batra, A.; Thulkar, S.; Julka, P.K. Leiomyosarcoma of pancreas: Imaging features. Indian. J. Gastroenterol. 2000, 19, 187–188. [Google Scholar]
- Ishikawa, O.; Matsui, Y.; Aoki, Y.; Iwanaga, T.; Terasawa, T.; Wada, A. Leiomyosarcoma of the pancreas. Report of a case and review of the literature. Am. J. Surg. Pathol. 1981, 5, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Riddle, N.D.; Quigley, B.C.; Browarsky, I.; Bui, M.M. Leiomyosarcoma arising in the pancreatic duct: A case report and review of the current literature. Case Rep. Med. 2010, 2010, 252364. [Google Scholar] [CrossRef]
- Kocakoc, E.; Havan, N.; Bilgin, M.; Atay, M. Primary pancreatic leiomyosarcoma. Iran. J. Radiol. 2014, 11, e4880. [Google Scholar] [CrossRef]
- Machado, M.C.; Cunha, J.E.; Penteado, S.; Bacchella, T.; Jukemura, J.; Costa, A.C.; Halpern-Salomon, I. Preoperative diagnosis of pancreatic leiomyosarcoma. Int. J. Pancreatol. 2000, 28, 97–100. [Google Scholar] [CrossRef]
- de la Santa, L.G.; Retortillo, J.A.; Miguel, A.C.; Klein, L.M. Radiology of pancreatic neoplasms: An update. World J. Gastrointest. Oncol. 2014, 6, 330–343. [Google Scholar] [CrossRef]
- Viúdez, A.; De Jesus-Acosta, A.; Carvalho, F.L.; Vera, R.; Martín-Algarra, S.; Ramírez, N. Pancreatic neuroendocrine tumors: Challenges in an underestimated disease. Crit. Rev. Oncol. Hematol. 2016, 101, 193–206. [Google Scholar] [CrossRef]
- Okun, S.D.; Lewin, D.N. Non-neoplastic pancreatic lesions that may mimic malignancy. Semin. Diagn. Pathol. 2016, 33, 31–42. [Google Scholar] [CrossRef]
- Konstantinidis, I.T.; Dursun, A.; Zheng, H.; Wargo, J.A.; Thayer, S.P.; Fernandez-del Castillo, C.; Warshaw, A.L.; Ferrone, C.R. Metastatic tumors in the pancreas in the modern era. J. Am. Coll. Surg. 2010, 211, 749–753. [Google Scholar] [CrossRef] [PubMed]
- Ogura, T.; Masuda, D.; Kurisu, Y.; Miyamoto, Y.; Hayashi, M.; Imoto, A.; Takii, M.; Takeuchi, T.; Inoue, T.; Tokioka, S.; et al. Multiple metastatic leiomyosarcoma of the pancreas: A first case report and review of the literature. Intern. Med. 2013, 52, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Wang, L.; Sheng, J.; Zhang, D.; Guan, L.; Zhao, K.; Zhang, X. Transdifferentiation of pancreatic stromal tumor into leiomyosarcoma with metastases to liver and peritoneum: A case report. BMC Cancer 2016, 16, 947. [Google Scholar] [CrossRef] [PubMed]
- Hébert-Magee, S.; Varadarajulu, S.; Frost, A.R.; Ramesh, J. Primary pancreatic leiomyosarcoma: A rare diagnosis obtained by EUS-FNA cytology. Gastrointest. Endosc. 2014, 80, 361–362. [Google Scholar] [CrossRef]
- Aihara, H.; Kawamura, Y.J.; Toyama, N.; Mori, Y.; Konishi, F.; Yamada, S. A small leiomyosarcoma of the pancreas treated by local excision. HPB 2002, 4, 145–148. [Google Scholar] [CrossRef]
- Milanetto, A.C.; Liço, V.; Blandamura, S.; Pasquali, C. Primary leiomyosarcoma of the pancreas: Report of a case treated by local excision and review of the literature. Surg. Case Rep. 2015, 1, 98. [Google Scholar] [CrossRef]
- Hur, Y.H.; Kim, H.H.; Park, E.K.; Seoung, J.S.; Kim, J.W.; Jeong, Y.Y.; Lee, J.H.; Koh, Y.S.; Kim, J.C.; Kim, H.J.; et al. Primary leiomyosarcoma of the pancreas. J. Korean Surg. Soc. 2011, 81 (Suppl. 1), S69–S73. [Google Scholar] [CrossRef]
- Izumi, H.; Okada, K.; Imaizumi, T.; Hirabayashi, K.; Matsuyama, M.; Dowaki, S.; Tobita, K.; Makuuchi, H. Leiomyosarcoma of the pancreas: Report of a case. Surg. Today 2011, 41, 1556–1561. [Google Scholar] [CrossRef]
- Battula, N.; Srinivasan, P.; Prachalias, A.; Rela, M.; Heaton, N. Primary pancreatic lymphoma: Diagnostic and therapeutic dilemma. Pancreas 2006, 33, 192–194. [Google Scholar] [CrossRef]
- Kloppel, G.; Solcia, E.; Longnecker, D.S.; Capella, C.; Sobin, L.H. Histological Typing of Tumours of the Exocrine Pancreas; World Health Organization International Classification of Tumours; Springer: Berlin, Germany, 1996; pp. 11–20. [Google Scholar]
- Sadot, E.; Yahalom, J.; Do, R.K.; Teruya-Feldstein, J.; Allen, P.J.; Gönen, M.; D’Angelica, M.I.; Kingham, T.P.; Jarnagin, W.R.; DeMatteo, R.P. Clinical features and outcome of primary pancreatic lymphoma. Ann. Surg. Oncol. 2015, 22, 1176–1184. [Google Scholar] [CrossRef]
- Jones, W.F.; Sheikh, M.Y.; McClave, S.A. AIDS-related non-Hodgkin’s lymphoma of the pancreas. Am. J. Gastroenterol. 1997, 92, 335–338. [Google Scholar]
- Facchinelli, D.; Sina, S.; Boninsegna, E.; Borin, A.; Tisi, M.C.; Piazza, F.; Scapinello, G.; Maiolo, E.; Hohaus, S.; Zamò, A.; et al. Primary pancreatic lymphoma: Clinical presentation, diagnosis, treatment, and outcome. Eur. J. Haematol. 2020, 105, 468–475. [Google Scholar] [CrossRef]
- Rad, N.; Khafaf, A.; Mohammad Alizadeh, A.H. Primary pancreatic lymphoma: What we need to know. J. Gastrointest. Oncol. 2017, 8, 749–757. [Google Scholar] [CrossRef]
- Mishra, M.V.; Keith, S.W.; Shen, X.; Ad, V.B.; Champ, C.E.; Biswas, T. Primary pancreatic lymphoma. Am. J. Clin. Oncol. 2013, 36, 38–43. [Google Scholar] [CrossRef]
- Fujinaga, Y.; Lall, C.; Patel, A.; Matsushita, T.; Sanyal, R.; Kadoya, M. MR features of primary and secondary malignant lymphoma of the pancreas: A pictorial review. Insights Imaging 2013, 4, 321–329. [Google Scholar] [CrossRef]
- Merkle, E.M.; Bender, G.N.; Brambs, H.J. Imaging findings in pancreatic lymphoma: Differential aspects. Am. J. Roentgenol. 2000, 174, 671–675. [Google Scholar] [CrossRef]
- Segaran, N.; Sandrasegaran, K.; Devine, C.; Wang, M.X.; Shah, C.; Ganeshan, D. Features of primary pancreatic lymphoma: A bi-institutional review with an emphasis on typical and atypical imaging features. World J. Clin. Oncol. 2021, 12, 823–832. [Google Scholar] [CrossRef]
- Low, G.; Panu, A.; Millo, N.; Leen, E. Multimodality imaging of neoplastic and nonneoplastic solid lesions of the pancreas. RadioGraphics 2011, 31, 993–1015. [Google Scholar] [CrossRef]
- Amodio, J.; Brodsky, J.E. Pediatric Burkitt lymphoma presenting as acute pancreatitis: MRI characteristics. Pediatr. Radiol. 2010, 40, 770–772. [Google Scholar] [CrossRef]
- Boninsegna, E.; Zamboni, G.A.; Facchinelli, D.; Triantopoulou, C.; Gourtsoyianni, S.; Ambrosetti, M.C.; Veneri, D.; Ambrosetti, A.; Pozzi Mucelli, R. CT imaging of primary pancreatic lymphoma: Experience from three referral centres for pancreatic diseases. Insights Imaging 2018, 9, 17–24. [Google Scholar] [CrossRef]
- Anand, D.; Lall, C.; Bhosale, P.; Ganeshan, D.; Qayyum, A. Current update on primary pancreatic lymphoma. Abdom. Radiol. 2016, 41, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.; Dang, N.; Dhawan, M.; Kulkarni, A. Diagnosis of a patient with primary pancreatic lymphoma. Gastroenterol. Hepatol. 2012, 8, 850–852. [Google Scholar]
- Saif, M.W. Primary pancreatic lymphomas. J. Pancreas 2006, 7, 262–273. [Google Scholar]
- Behrns, K.E.; Sarr, M.G.; Strickler, J.G. Pancreatic lymphoma: Is it a surgical disease? Pancreas 1994, 9, 662–667. [Google Scholar] [CrossRef]
- Sadaf, S.; Loya, A.; Akhtar, N.; Yusuf, M.A. Role of endoscopic ultrasound guided-fine needle aspiration biopsy in the diagnosis of lymphoma of the pancreas: A clinicopathological study of nine cases. Cytopathology 2017, 28, 536–541. [Google Scholar] [CrossRef]
- Freeman, C.; Berg, J.W.; Cutler, S.J. Occurrence and prognosis of extranodal lymphomas. Cancer 1972, 29, 252–260. [Google Scholar] [CrossRef]
- Vitolo, U.; Seymour, J.F.; Martelli, M.; Illerhaus, G.; Illidge, T.; Zucca, E.; Campo, E.; Ladetto, M.; ESMO Guidelines Committee. Extranodal diffuse large B-cell lymphoma (DLBCL) and primary mediastinal B-cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27 (Suppl. 5), 91–102. [Google Scholar] [CrossRef] [PubMed]
- Ballarin, R.; Spaggiari, M.; Cautero, N.; De Ruvo, N.; Montalti, R.; Longo, C.; Pecchi, A.; Giacobazzi, P.; De Marco, G.; D’Amico, G.; et al. Pancreatic metastases from renal cell carcinoma: The state of the art. World J. Gastroenterol. 2011, 17, 4747–4756. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Wolfgang, C.L. The role of surgery in the management of isolated metastases to the pancreas. Lancet Oncol. 2009, 10, 287–293. [Google Scholar] [CrossRef]
- Reddy, S.; Edil, B.H.; Cameron, J.L.; Pawlik, T.M.; Herman, J.M.; Gilson, M.M.; Campbell, K.A.; Schulik, R.D.; Ahuja, N.; Wolfgang, C.L. Pancreatic resection of isolated metastases from nonpancreatic primary cancers. Ann. Surg. Oncol. 2008, 15, 3199–3206. [Google Scholar] [CrossRef]
- Sweeny, A.D.; Fisher, W.E.; Wu, M.F.; Hilsenbeck, S.G.; Brunicardi, F.C. Value of pancreatic resection for cancer metastatic to the pancreas. J. Surg. Res. 2010, 160, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Showalter, S.L.; Hager, E.; Yeo, C.J. Metastatic disease to the pancreas and spleen. Semin. Oncol. 2008, 35, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Rypens, F.; Van Gansbeke, D.; Lambilliotte, J.P.; Van Regemorter, G.; Verhest, A.; Struyven, J. Pancreatic metastasis from renal cell carcinoma. Br. J. Radiol. 1992, 65, 547–548. [Google Scholar] [CrossRef] [PubMed]
- Ferrozzi, F.; Bova, D.; Campodonico, F.; Chiara, F.D.; Passari, A.; Bassi, P. Pancreatic metastases: CT assessment. Eur. Radiol. 1997, 7, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Muranaka, T.; Teshima, K.; Honda, H.; Nanjo, T.; Hanada, K.; Oshiumi, Y. Computed tomography and histologic appearance of pancreatic metastases from distant sources. Acta Radiol. 1989, 30, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.K.; Chuah, K.L. Metastatic renal cell carcinoma to the pancreas: A review. Arch. Pathol. Lab. Med. 2016, 140, 598–602. [Google Scholar] [CrossRef]
- Sikka, A.; Adam, S.Z.; Wood, C.; Hoff, F.; Harmath, C.B.; Miller, F.H. Magnetic resonance imaging of pancreatic metastases from renal cell carcinoma. Clin. Imaging 2015, 39, 945–953. [Google Scholar] [CrossRef]
- Maeno, T.; Satoh, H.; Ishikawa, H.; Yamashita, Y.T.; Naito, T.; Fujiwara, M.; Kamma, H.; Ohtsuka, M.; Hasegawa, S. Patterns of pancreatic metastasis from lung cancer. Anticancer Res. 1998, 18, 2881–2884. [Google Scholar]
- Woo, J.S.; Joo, K.R.; Woo, Y.S.; Jang, J.Y.; Chang, Y.W.; Lee, J.I.; Chang, R. Pancreatitis from metastatic small cell lung cancer: Successful treatment with endoscopic intrapancreatic stenting. Korean J. Intern. Med. 2006, 21, 256. [Google Scholar] [CrossRef]
- Cwik, G.; Wallner, G.; Skoczylas, T.; Ciechanski, A.; Zinkiewicz, K. Cancer antigens 19-9 and 125 in the differential diagnosis of pancreatic mass lesions. Arch. Surg. 2006, 141, 968–973. [Google Scholar] [CrossRef]
- Okamoto, T. Malignant biliary obstruction due to metastatic non-hepato-pancreato-biliary cancer. World J. Gastroenterol. 2022, 28, 985–1008. [Google Scholar] [CrossRef] [PubMed]
- Ascenti, G.; Visalli, C.; Genitori, A.; Certo, A.; Pitrone, A.; Mazziotti, S. Multiple hypervascular pancreatic metastases from renal cell carcinoma: Dynamic MR and spiral CT in three cases. Clin. Imaging 2004, 28, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Galia, M.; Albano, D.; Picone, D.; Terranova, M.C.; Agrusa, A.; Di Buono, G.; Licata, A.; Lo Re, G.; La Grutta, L.; Midiri, M. Imaging features of pancreatic metastases: A comparison with pancreatic ductal adenocarcinoma. Clin. Imaging 2018, 51, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Kelekis, N.L.; Semelka, R.C.; Siegelman, E.S. MRI of pancreatic metastases from renal cancer. J. Comput. Assist. Tomogr. 1996, 20, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Crippa, S.; Angelini, C.; Mussi, C.; Bonardi, C.; Romano, F.; Sartori, P.; Uggeri, F.; Bovo, G. Surgical treatment of metastatic tumors to the pancreas: A single center experience and re-view of the literature. World J. Surg. 2006, 30, 1536–1542. [Google Scholar] [CrossRef]
- Sperti, C.; Pasquali, C.; Liessi, G.; Pinciroli, L.; Decet, G.; Pedrazzoli, S. Pancreatic resection for metastatic tumors to the pancreas. J. Surg. Oncol. 2003, 83, 161–166. [Google Scholar] [CrossRef]
- Law, C.H.; Wei, A.C.; Hanna, S.S.; Al-Zahrani, M.; Taylor, B.R.; Greig, P.D.; Langer, B.; Gallinger, S. Pancreatic resection for metastatic renal cell carcinoma: Presentation, treatment, and outcome. Ann. Surg. Oncol. 2003, 10, 922–926. [Google Scholar] [CrossRef]
- Scatarige, J.C.; Horton, K.M.; Sheth, S.; Fishman, E.K. Pancreatic parenchymal metastases: Observations on helical CT. Am. J. Roentgenol. 2001, 176, 695–699. [Google Scholar] [CrossRef]
- Atlas, S.W.; Braffmann, B.H.; LoBrutto, R.; Elder, D.E.; Herlyn, D. Human malignant melanomas with varying degrees of melanin content in nude mice: MR imaging, histopathology, and electron paramagnetic resonance. J. Comput. Assist. Tomogr. 1990, 14, 547–554. [Google Scholar] [CrossRef]
- Wang, H.; Nie, P.; Dong, C.; Li, J.; Huang, Y.; Hao, D.; Xu, W. CT and MRI Findings of Soft Tissue Adult Fibrosarcoma in Extremities. Biomed. Res. Int. 2018, 2018, 6075705. [Google Scholar] [CrossRef]
- Adsay, N.V.; Andea, A.; Basturk, O.; Kilinc, N.; Nassar, H.; Cheng, J.D. Secondary tumors of the pancreas: An analysis of a surgical and autopsy database and review of the literature. Virchows Arch. 2004, 444, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.H.; Tamm, E.P.; Marcal, L.; Balachandran, A.; Charnsangavej, C.; Vikram, R.; Bhosale, P. Imaging features of hematogenous metastases to the pancreas: Pictorial essay. Cancer Imaging 2011, 11, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Palmowski, M.; Hacke, N.; Satzl, S.; Klauss, M.; Wente, M.N.; Neukamm, M.; Kleeff, J.; Hallscheidt, P. Metastasis to the pancreas: Characterization by morphology and contrast enhancement features on CT and MRI. Pancreatology 2008, 8, 199–203. [Google Scholar] [CrossRef]
- Bahra, M.; Jacob, D.; Langrehr, J.M.; Glanemann, M.; Schumacher, G.; Lopez-Hänninen, E.; Neuhaus, P. Metastasen im Pankreas. Wann ist eine Resektion sinnvoll? Chirurg 2008, 79, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Bassi, C.; Butturini, G.; Falconi, M.; Sargenti, M.; Mantovani, W.; Pederzoli, P. High recurrence rate after atypical resection for pancreatic metastases from renal cell carcinoma. Br. J. Surg. 2003, 90, 555–559. [Google Scholar] [CrossRef] [PubMed]

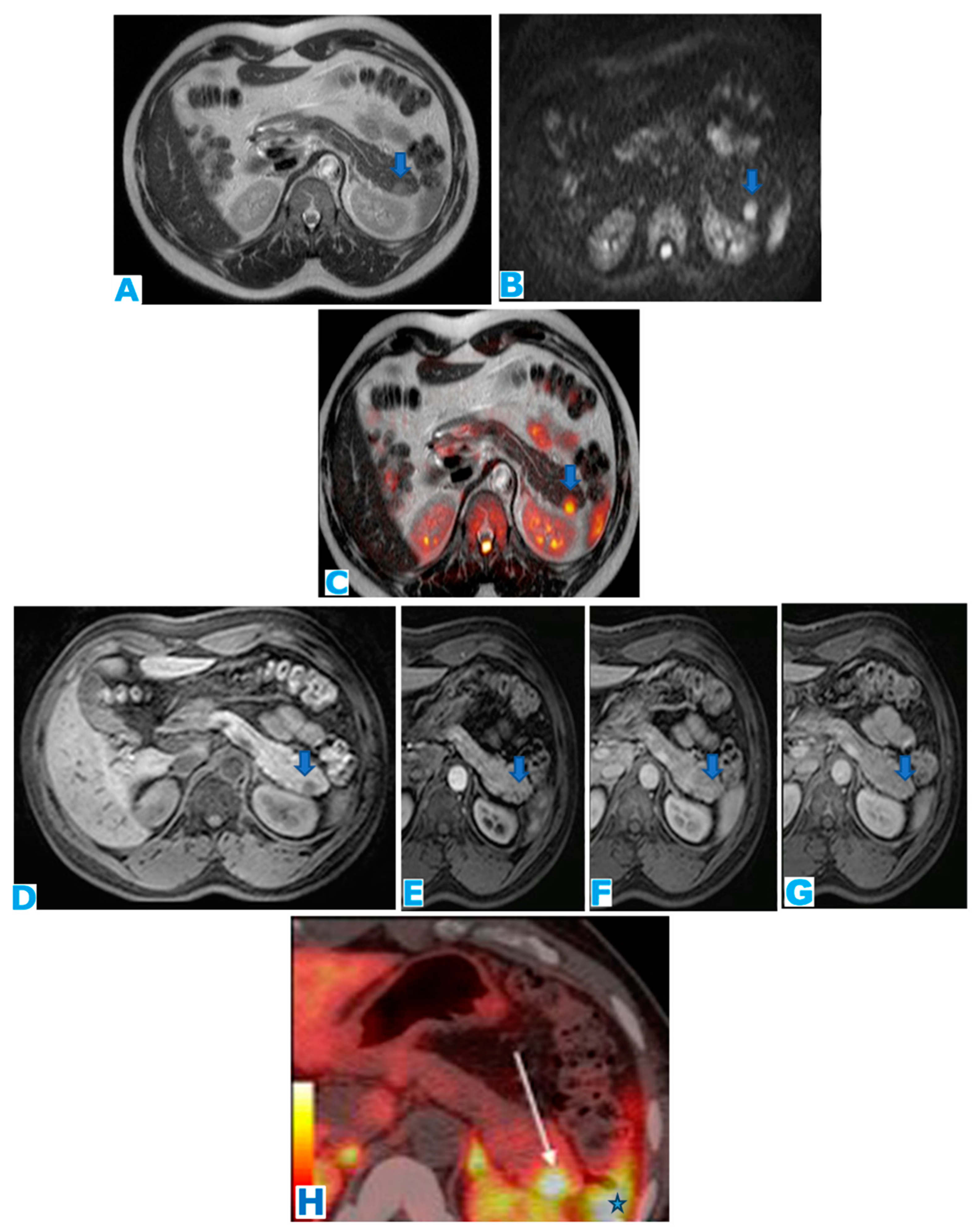{kind=link}
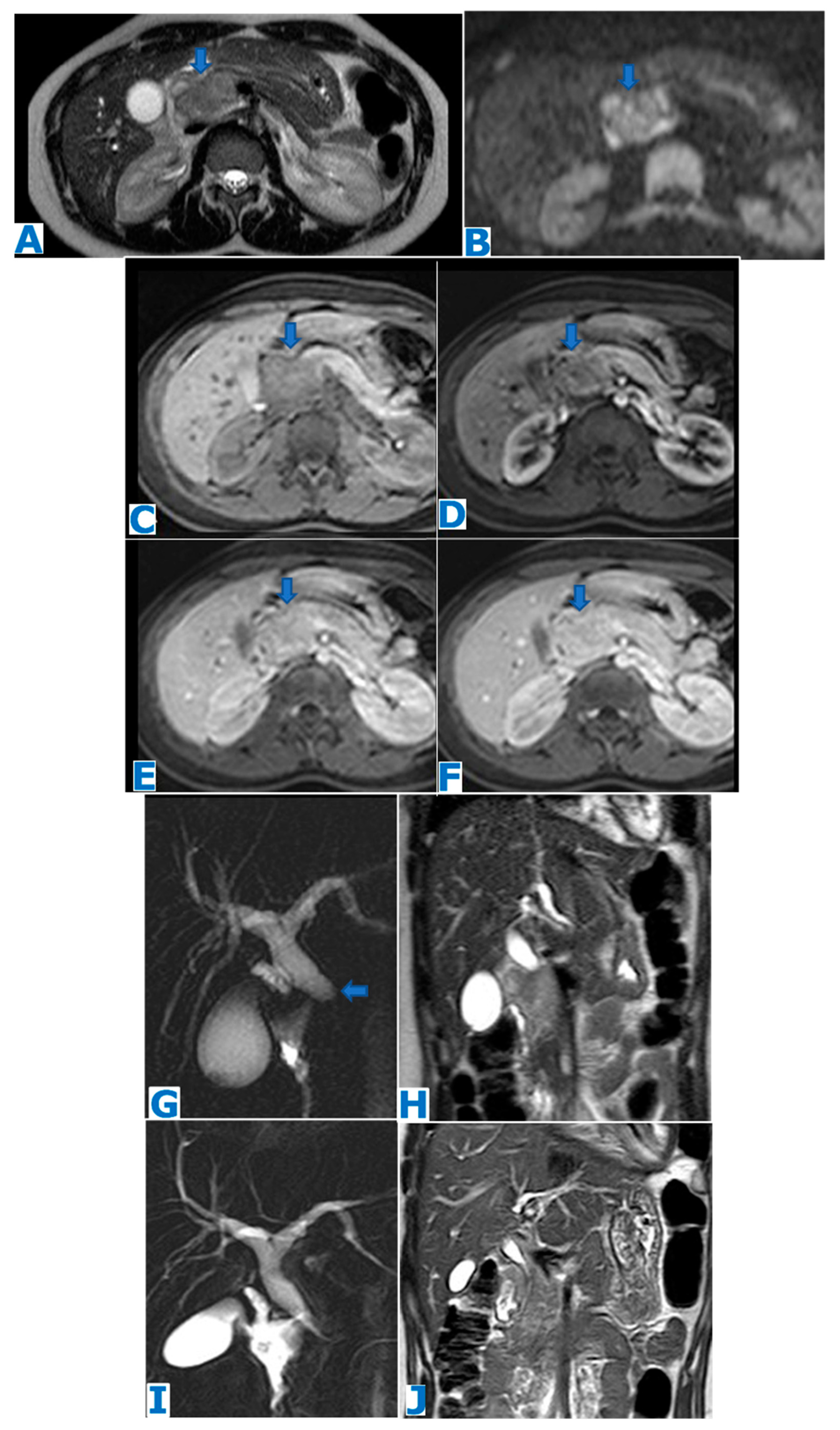{kind=link}
{kind=link}
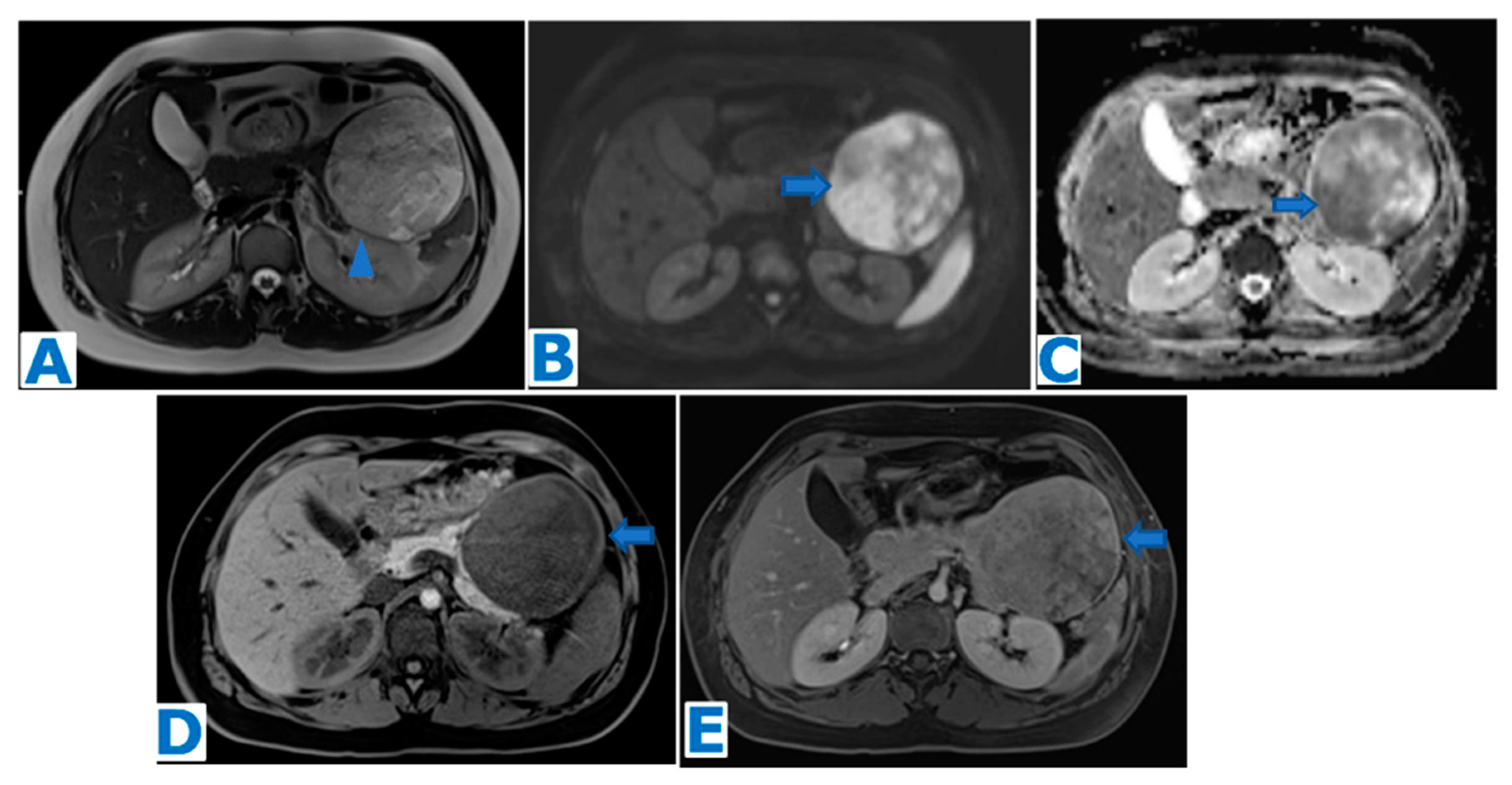{kind=link}
{kind=link}
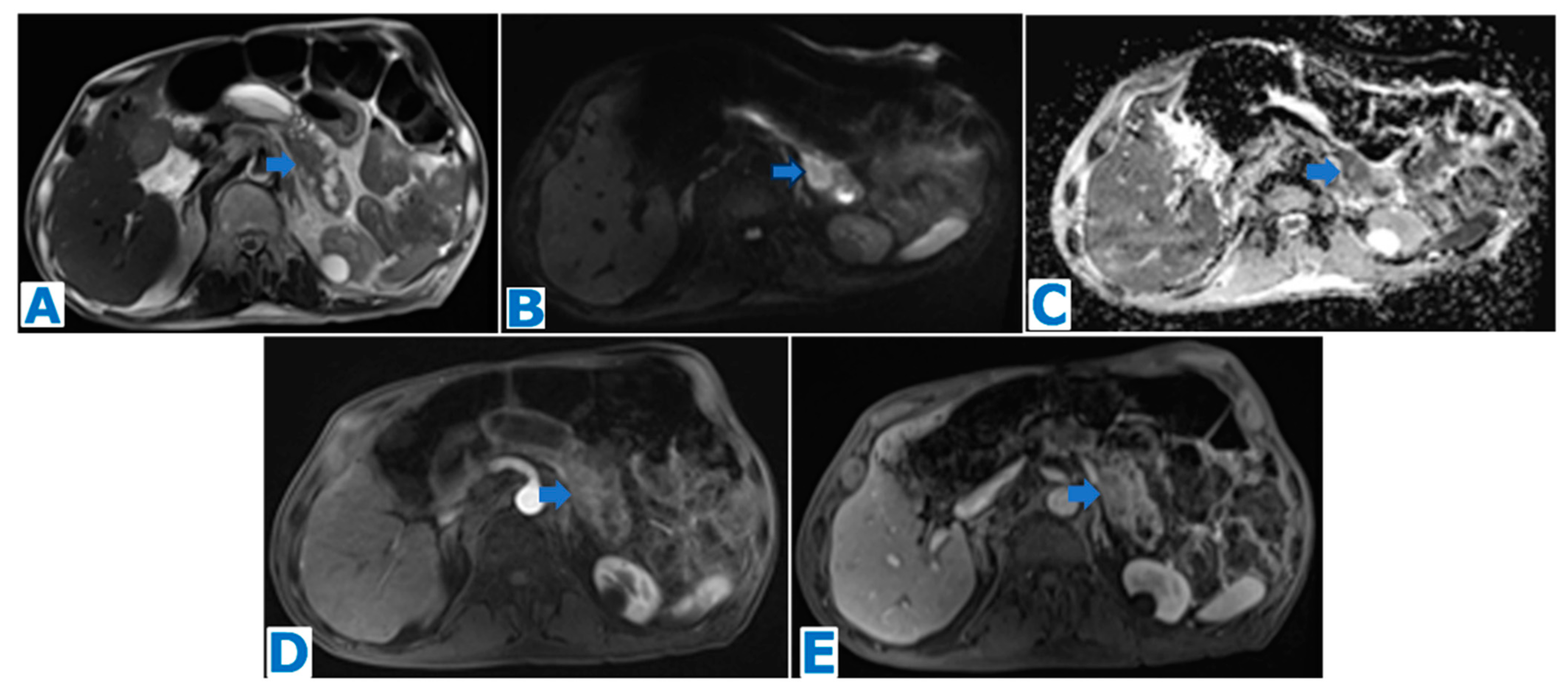{kind=link}
{kind=link}
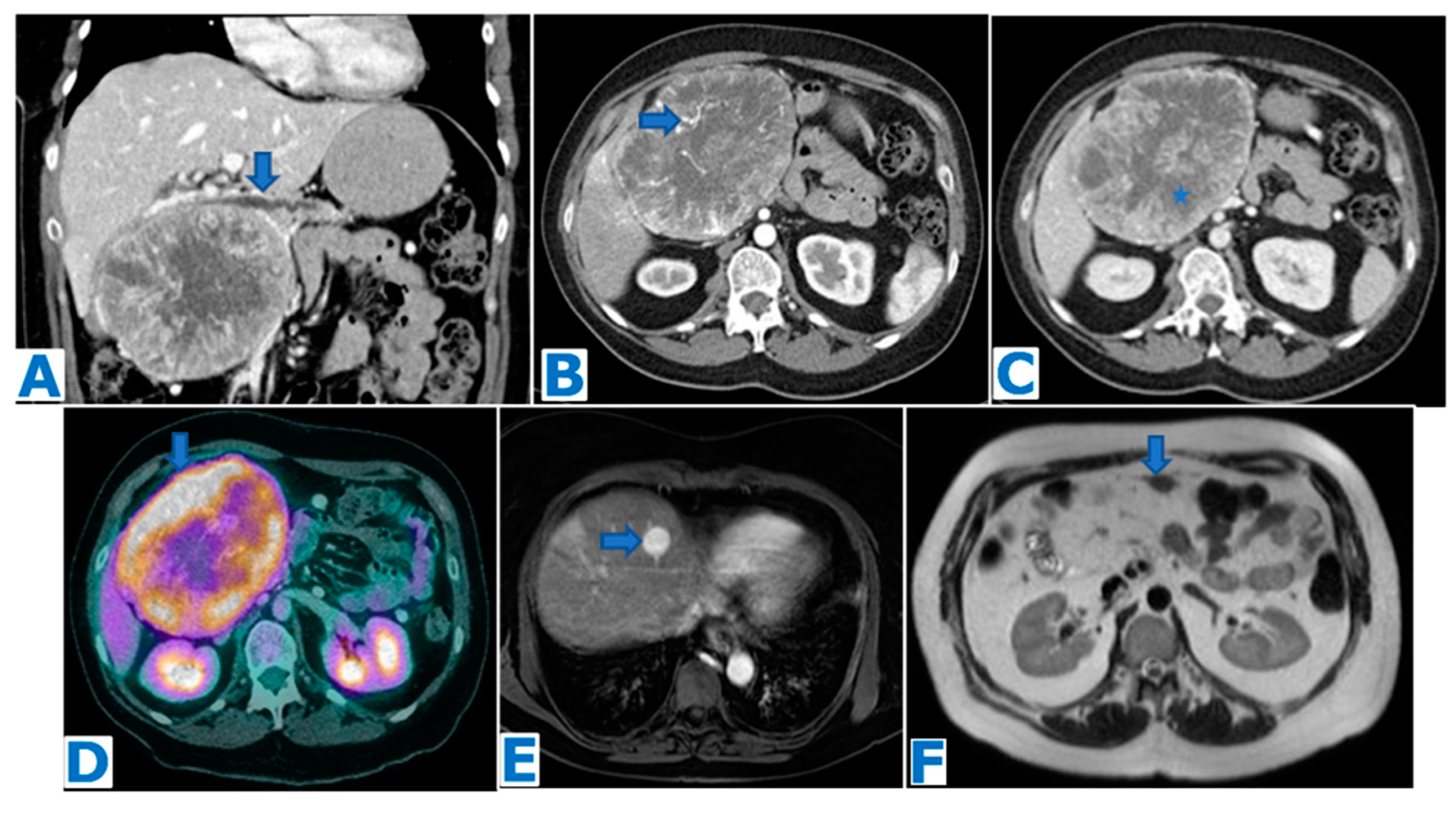{kind=link}
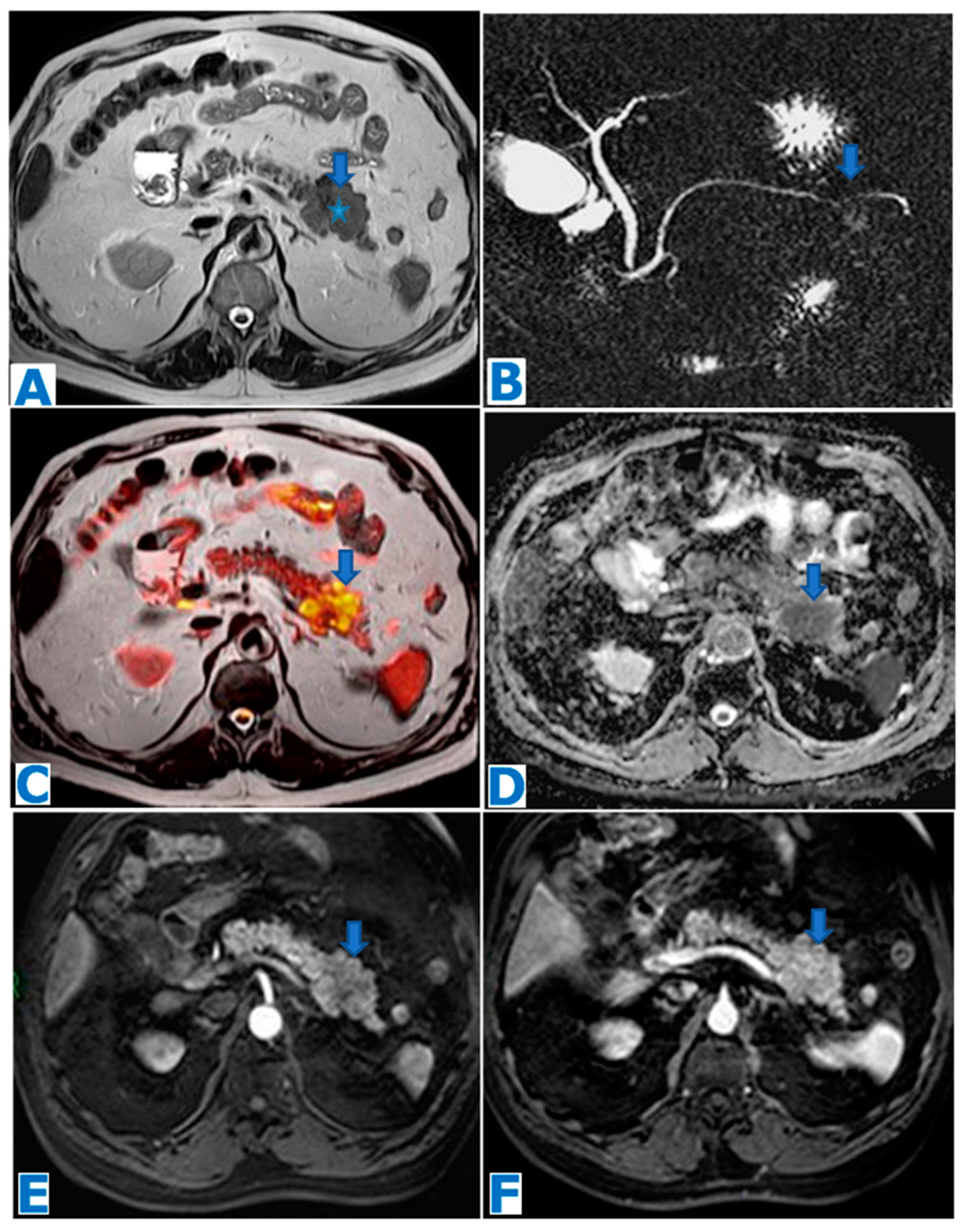{kind=link}
{kind=link}
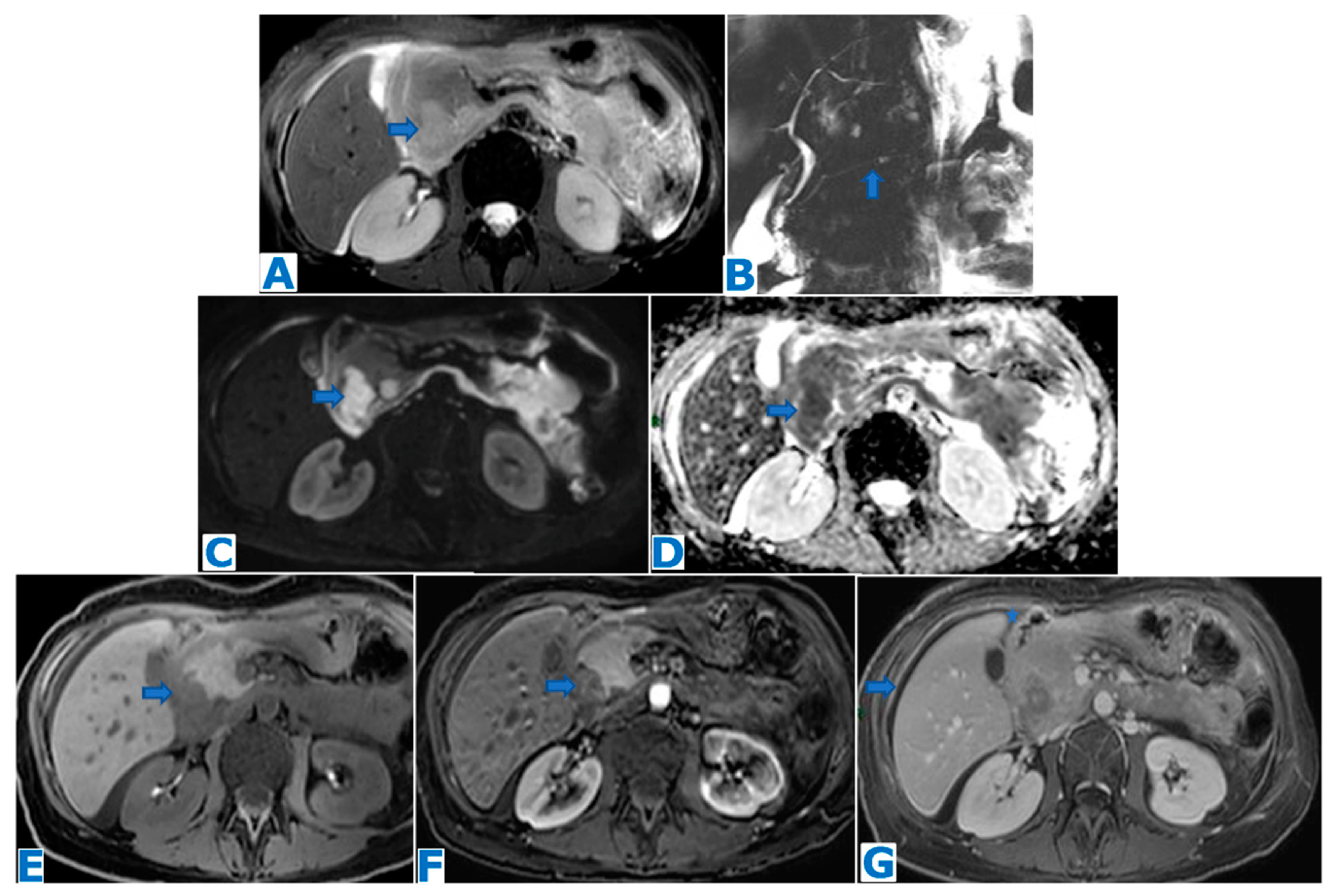{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
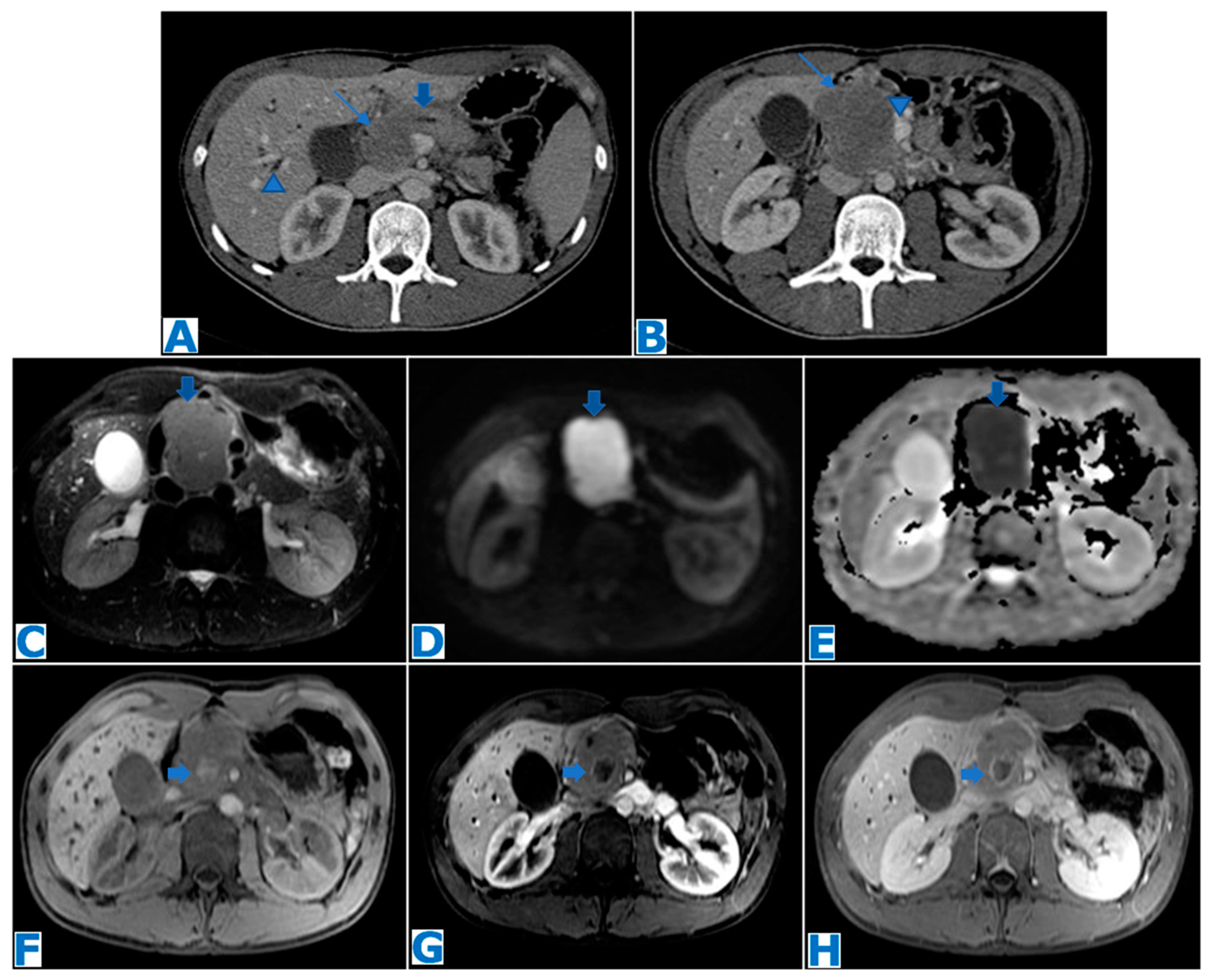{kind=link}
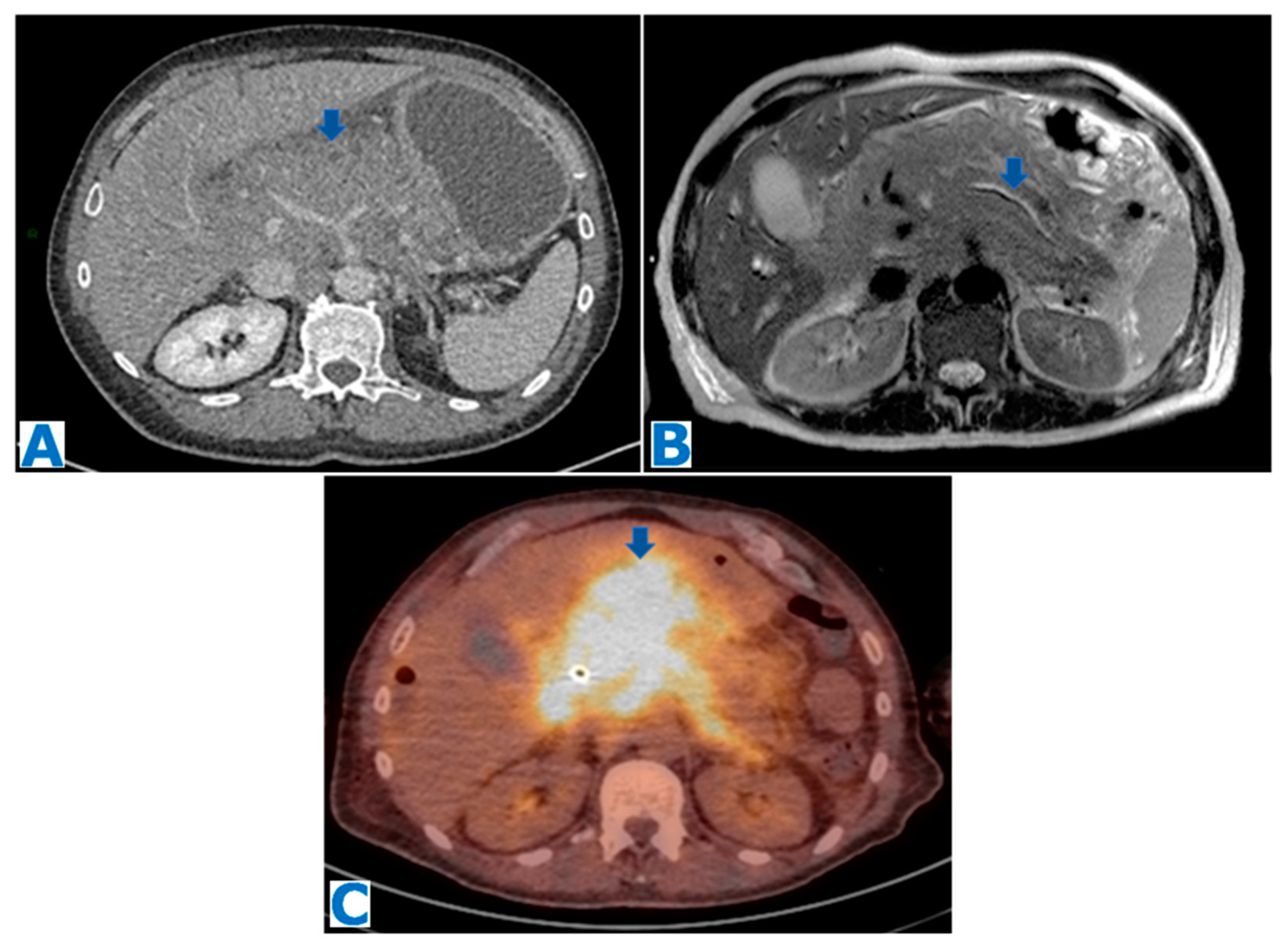{kind=link}
{kind=link}
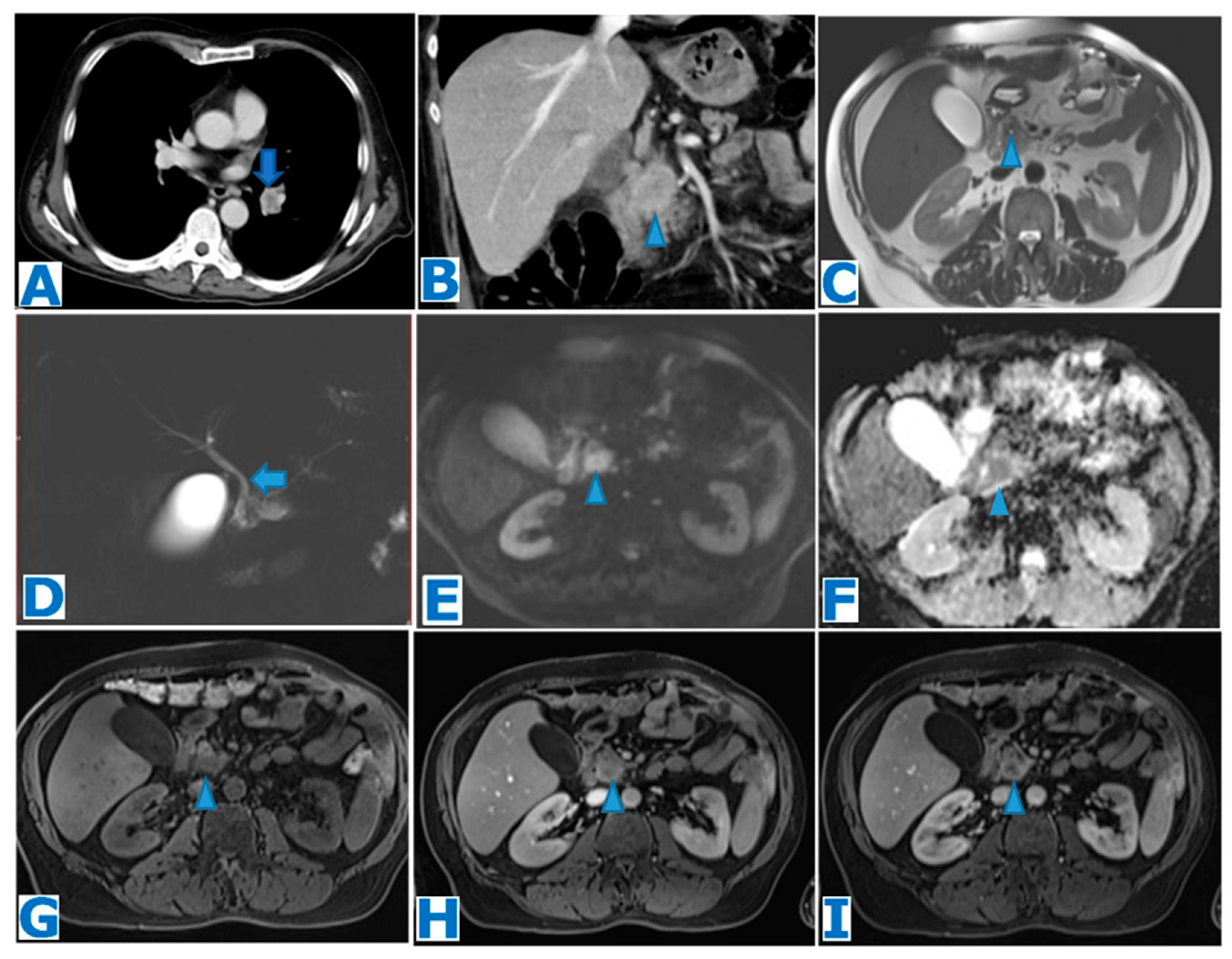{kind=link}
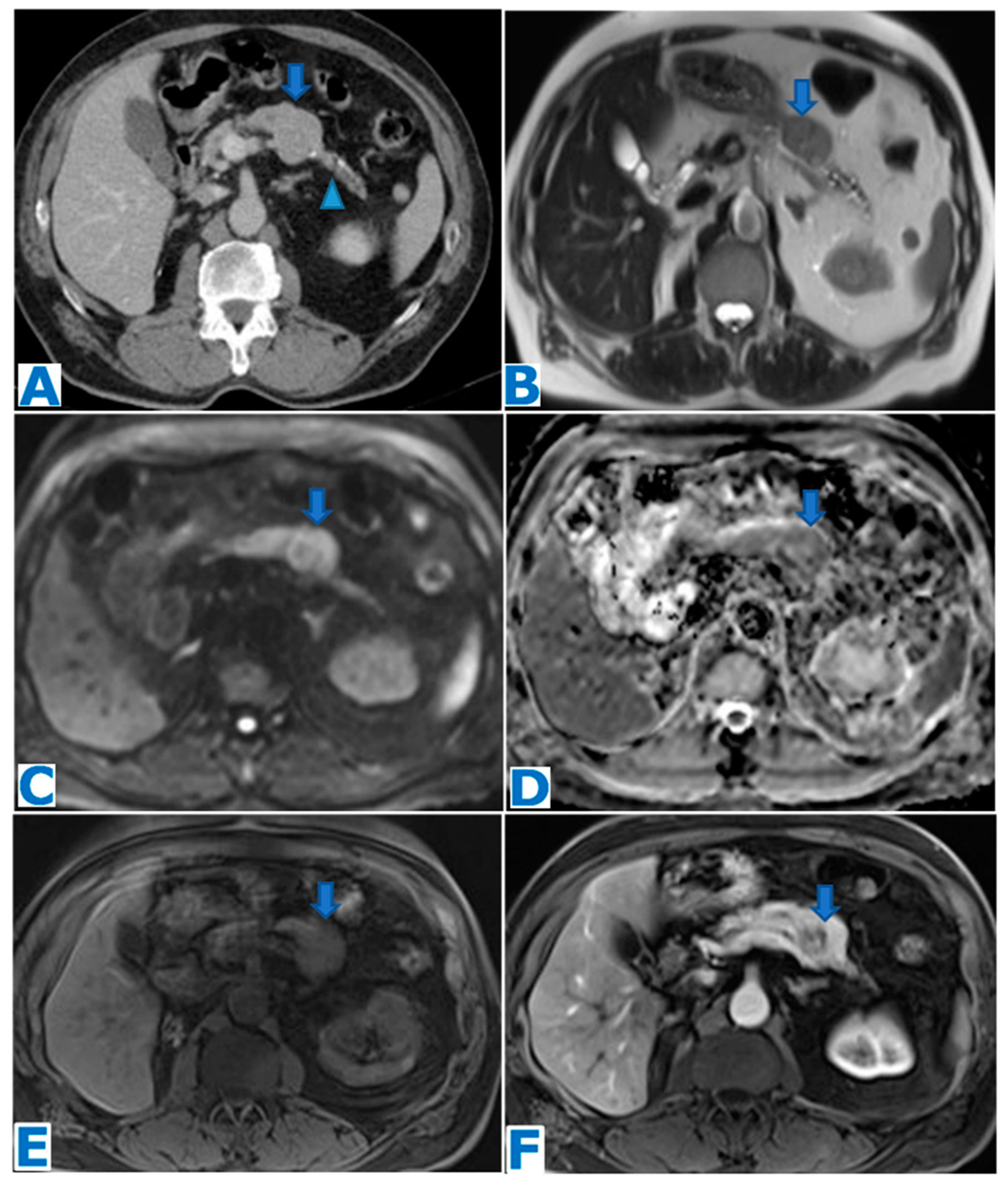{kind=link}
{kind=link}
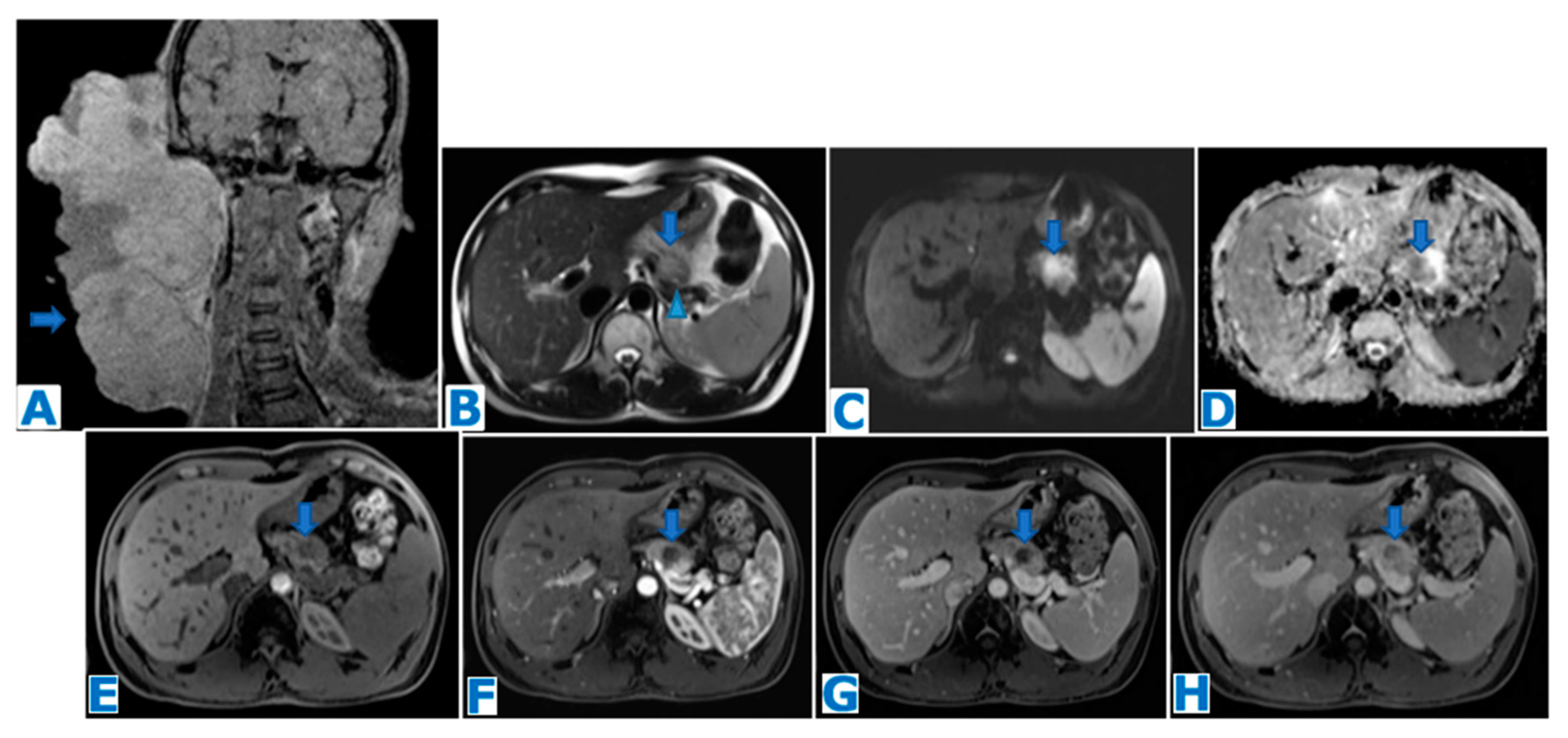{kind=link}
Table 1.
Classification of rare solid pancreatic lesions.
| Benign | Potentially Malignant | Malignant |
|---|---|---|
| Intrapancreatic splenic tissue | Solid pseudopapillary tumour | Acinar cell carcinoma |
| Tuberculosis | Schwannoma | Undifferentiated carcinoma with osteoclastic-like giant cells. |
| Solid serous cystadenoma | Purely intraductal neuroendocrine tumour | Adenosquamous carcinoma |
| Fibrous solitary tumour | Colloid carcinoma | |
| Primary leiomyosarcoma | ||
| Lymphoma (primary and secondary) | ||
| Metastases |
Table 2.
No. of cases/incidence/prevalence of rare solid pancreatic lesions depicted.
| Rare Solid Pancreatic Lesions | No. of Cases/Incidence/Prevalence |
|---|---|
| Intrapancreatic splenic tissue | 61 cases/3000 autopsies |
| Tuberculosis | 116 cases |
| Solid serous cystadenoma | 22 cases |
| Solid pseudopapillary tumour | 2% of all exocrine pancreatic neoplasms |
| Schwannoma | <80 cases reported |
| Purely intraductal neuroendocrine tumour | 7 cases reported |
| Fibrous solitary tumour | 29 cases reported |
| Acinar cell carcinoma | <2% of all primary pancreatic neoplasms |
| Undifferentiated carcinoma with osteoclasic-like giant cells | <1% of all malignant pancreatic neoplasms |
| Adenosquamous carcinoma | 0.38–10% prevalence |
| Colloid carcinoma | 1% of all pancreatic tumours |
| Primary leiomyosarcoma | 0.1% of malignant pancreatic neoplasms |
| Primary lymphoma | <0.5% of all primary pancreatic neoplasms, 1% of all extranodal lymphomas |
| Secondary lymphoma | 30% cases of extranodal lymphoma |
| Metastases | 2–5% of pancreatic malignancies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Veron Sanchez, A.; Santamaria Guinea, N.; Cayon Somacarrera, S.; Bennouna, I.; Pezzullo, M.; Bali, M.A. Rare Solid Pancreatic Lesions on Cross-Sectional Imaging. Diagnostics 2023, 13, 2719. https://doi.org/10.3390/diagnostics13162719
AMA Style
Veron Sanchez A, Santamaria Guinea N, Cayon Somacarrera S, Bennouna I, Pezzullo M, Bali MA. Rare Solid Pancreatic Lesions on Cross-Sectional Imaging. Diagnostics. 2023; 13(16):2719. https://doi.org/10.3390/diagnostics13162719
Chicago/Turabian StyleVeron Sanchez, Ana, Nuria Santamaria Guinea, Silvia Cayon Somacarrera, Ilias Bennouna, Martina Pezzullo, and Maria Antonietta Bali. 2023. "Rare Solid Pancreatic Lesions on Cross-Sectional Imaging" Diagnostics 13, no. 16: 2719. https://doi.org/10.3390/diagnostics13162719
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.