
Male Involvement in Family Planning Decisions in Malawi and Tanzania: What Are the Determinants?


Abstract
:1. Introduction
2. Methods
2.1. Data Source and Sampling Procedures
2.2. Study Variables and Measurements
2.2.1. Outcome Variable
2.2.2. Independent Variables
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. Socio-Demographic Characteristics of the Respondents in Malawi and Tanzania
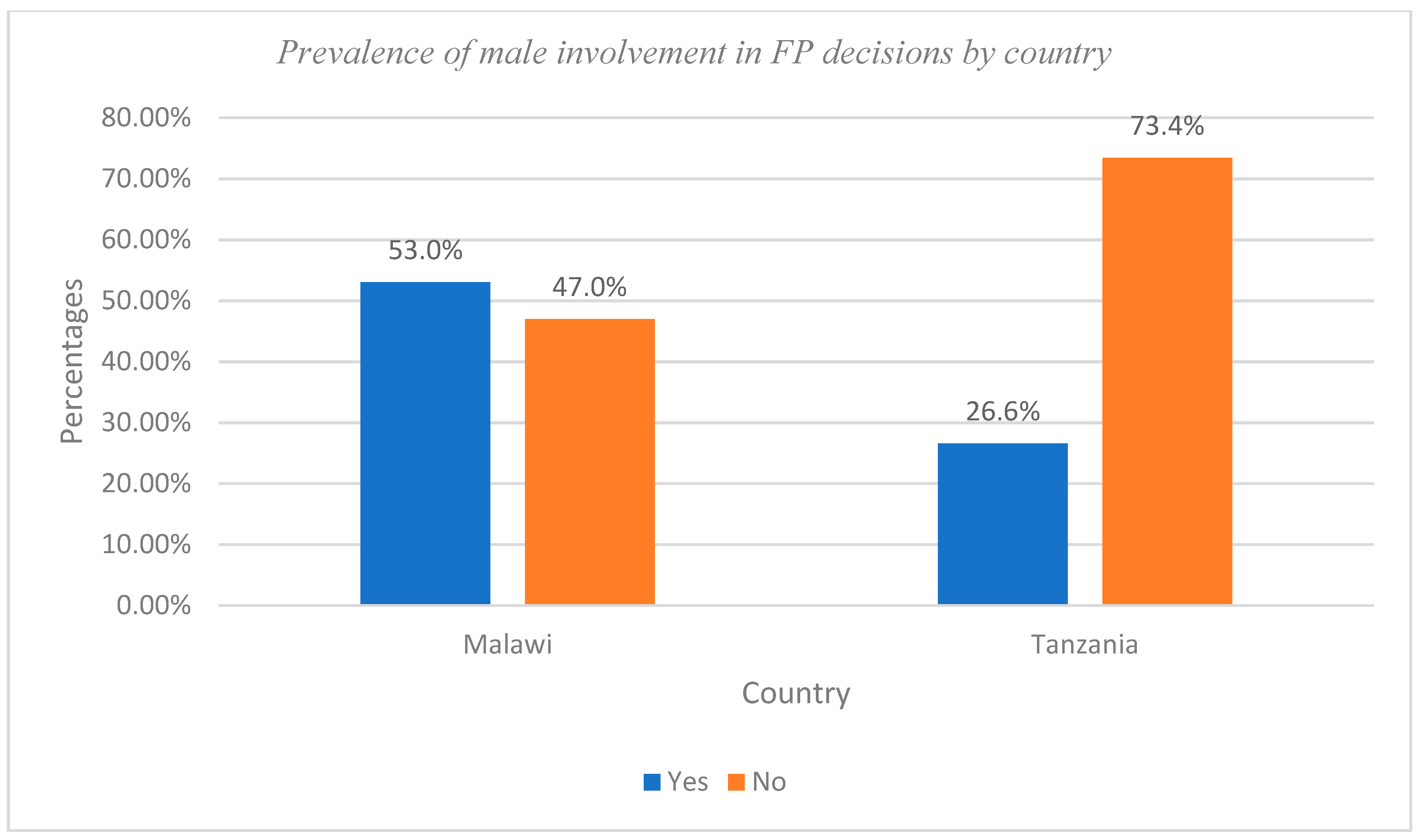
3.2. Prevalence of Involvement in FP Decisions by Countries
3.3. Male Involvement in FP Decisions Associated with Characteristics of the Respondents
3.4. Determinants Associated with Male Involvement in FP Decisions
4. Discussion
5. Male Involvement in Family Planning and Its Implications for 2030 Agenda for SDG 3
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akokuwebe, M.E. Breastfeeding as a form of contraceptive among nursing mothers in Ibadan, Nigeria. Afr. J. Psychol. Study Soc. Issues 2014, 17, 39–57. [Google Scholar]
- Akokuwebe, M.E.; Okafor, E.E. Maternal health and the implications for sustainable transformation in Nigeria. Res. Humanit. Soc. Sci. 2015, 5, 1–13. [Google Scholar]
- Vouking, M.Z.; Evina, C.D.; Tadenfok, C.N. Male involvement in family planning decision-making in sub-Saharan Africa—What the evidence suggests. Pan Afr. Med. J. 2014, 19, 349. [Google Scholar] [CrossRef]
- Sait, M.; Ajarbou, A.; Almannie, R.; Binsaleh, S. Knowledge, attitudes, and perception patterns of contraception methods. Urol. Ann. 2021, 13, 243–253. [Google Scholar]
- Tamiso, A.; Tassew, A.; Bekele, H.; Zemede, Z.; Dulla, A. Barriers to males involvement in family planning services in Arba Minch Town, Southern Ethiopia: Qualitative case study. Int. J. Public Health Sci. 2016, 5, 46–50. [Google Scholar]
- Aventin, A.; Robinson, M.; Hanratty, J.; Ruane-McAteer, E.; Tomlinson, M.; Clarke, M.; Okonofua, F.; Bonell, C.; Lohan, M. PROTOCOL: Involving men and boys in family planning: A systematic review of the effective components and characteristics of complex interventions in low- and middle-income countries. Campbell Syst. Rev. 2021, 17, e1140. [Google Scholar] [CrossRef]
- Adedemiji, A.A.; Akokuwebe, M.E.; Omololu, O.O. Use of lactational amenorrhea method (LAM) as contraception among women in Ibadan, Nigeria. J. Environ. Cult. 2013, 10, 39–61. [Google Scholar]
- Omololu, O.G.; Akokuwebe, M.E. Knowledge and practice of exclusive breastfeeding as a contraceptive form among childbearing women in Ibadan, Nigeria. Afr. J. Psychol. Study Soc. Issues 2014, 17, 3–15. [Google Scholar]
- Kabagenyi, A.; Jennings, L.; Reid, A.; Nalwadda, G.; Ntozi, J.; Atuyambe, L. Barriers to male involvement in contraceptive uptake and reproductive health services: A qualitative study of men and women’s perceptions in two rural districts in Uganda. Reprod. Health 2014, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- Makoni, A.; Chemhuru, M.; Chimbetete, C.; Gombe, W.; Mungati, M.; Bangure, D.; Tshimanga, M. Factors associated with male involvement in the prevention of mother-to-child transmission of HIV, Midlands Province, Zimbabwe, 2015—A case control study. BMC Public Health 2016, 16, 331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akokuwebe, M.E.; Falayi, E.O.; Adekola, F.; Saliu, M.Y. Sexual behaviour of in-school rural adolescents in Ogun State, Nigeria. Afr. J. Biomed. Res. 2019, 22, 135–143. [Google Scholar]
- Tokhi, M.; Comrie-Thomson, L.; Davis, J.; Portela, A.; Chersich, M.; Luchters, S. Involving men to improve maternal and newborn health: A systematic review of the effectiveness of interventions. PLoS ONE 2018, 13, e0191620. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). WHO Updates Recommendations to Guide Family Planning Decisions. WHO. 2022. Available online: https://www.who.int/news/item/15-11-2022-who-updates-recommendations-to-guide-family-planning-decisions (accessed on 3 January 2023).
- Akokuwebe, M.E.; Olasoju, M.O. Socio-demographic factors affecting the use of maternal health service in rural Ondo Nigeria. Ib. J. Soc. Sci. 2016, 14, 119–134. [Google Scholar]
- Amusan, L.; Akokuwebe, M.E. Conceptualising Afrocentric-feminism and social constructivism through Alma Ata Declaration (primary health care, PHC) in rural Nigeria. Gend. Behav. 2016, 14, 7246–7253. [Google Scholar]
- Akokuwebe, M.E.; Sasona, S.J.; Adetayo, B.C. Factors Responsible for Adolescent Pregnancy in Rural Areas of Ife North LGA, Osun State. Centrepoint J. (Humanit. Ed.) Univ. Ilorin 2018, 21, 1–28. [Google Scholar]
- Kriel, Y.; Milford, C.; Cordero, J.; Suleman, F.; Beksinska, M.; Steyn, P.; Smit, J.A. Male partner influence on family planning and contraceptive use: Perspectives from community members and healthcare providers in KwaZulu-Natal, South Africa. Reprod. Health 2019, 16, 89. [Google Scholar] [CrossRef] [Green Version]
- Machinda, Z.I.; Mbonile, M.J.; Mtae, H.G. Determinants of male involvement in family planning services in Tarime District, Tanzania. Tanzan. J. Popul. Stud. Dev. 2020, 27, 93–108. [Google Scholar]
- Lusambili, A.M.; Muriuki, P.; Wisofschi, S.; Shumba, C.S.; Mantel, M.; Obure, J.; Nyaga, L.; Mulama, K.; Ngugi, A.; Orwa, J.; et al. Male Involvement in Reproductive and Maternal and New Child Health: An Evaluative Qualitative Study on Facilitators and Barriers from Rural Kenya. Front. Public Health 2021, 9, 287. [Google Scholar] [CrossRef] [PubMed]
- Abrejo, F.G.; Shaikh, B.T.; Saleem, S. ICPD to MDGs: Missing links and common grounds. Reprod. Health 2008, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- Roseman, M.J.; Reichenbach, L. International Conference on population and development at 15 years: Achieving sexual and reproductive health and rights for all? Am. J. Public Health 2010, 100, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Nzioka, C. Factors Influencing Male Interest in Family Planning in Kenya. Afr. J. Reprod. Health/La Rev. Afr. La St. Reprod. 1998, 2, 122–141. [Google Scholar]
- Fapohunda, B.M.; Rutenberg, N. Expanding Men’s Participation in Reproductive Health in Kenya; African Population Policy Research Center: Nairobi, Kenya, 1999. [Google Scholar]
- Withers, M.; Dworkin, S.L.; Onono, M.; Oyier, B.; Cohen, C.R.; Bukusi, E.A.; Newmann, S.J. Men’s Perspectives on Their Role in Family Planning in Nyanza Province, Kenya. Stud. Fam. Plan. 2015, 46, 201–215. [Google Scholar] [CrossRef]
- Casey, F.E.; Sonenstein, F.L.; Astone, N.M.; Pleck, J.H.; Dariotis, J.K.; Marcell, A.V. Family planning and pre-conception health among men in their mid-30s: Developing indicators and describing need. Am. J. Men’s Health 2016, 10, 59–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishwajit, G.; Tang, S.; Yaya, S.; Ide, S.; Fu, H.; Wang, M.; He, Z.; Da, F.; Feng, Z. Factors associated with male involvement in reproductive care in Bangladesh. BMC Public Health 2017, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- Ani, F.; Abiodun, O.; Sotunsa, J.; Faturoti, O.; Imaralu, J.; Olaleye, A. Demographic factors related to male involvement in reproductive healthcare services in Nigeria. Eur. J. Contracept. Reprod. Health Care 2016, 21, 57–67. [Google Scholar] [CrossRef] [PubMed]
- National Population Commission. Nigeria Demographic and Health Survey 2018; The DHS Program; ICF: Rockville, MD, USA, 2019. [Google Scholar]
- Oyefabi, A.; Danbo, H.; Nwankwo, B.; Waje, C.; Kure, S.; AKabe, J. Determinants of male involvement in family planning decision making in a rural community in Northern Nigeria. J. Community Med. Prim. Health Care 2022, 34, 69–81. [Google Scholar] [CrossRef]
- Alhassan, N.; Madise, N.J. Demand for family planning satisfied with modern methods in urban Malawi: CHAID analysis to identify predictors and women underserved with family planning services. Front. Glob. Women’s Health 2021, 2, 652902. [Google Scholar] [CrossRef] [PubMed]
- Dral, A.A.; Tolani, M.R.; Smet, E.; van Luijn, A. Factors influencing male involvement in family planning in Ntchisi District, Malawi—A qualitative study. Afr. J. Reprod. Health 2018, 22, 35–43. [Google Scholar]
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC); Tanzania Mainland, Ministry of Health (MoH) [Zanzibar]; National Bureau of Statistics (NBS); Office of the Chief Government Statistician (OCGS); ICF. 2015–2016 TDHS-MIS Key Findings; MoHCDGEC; MoH; NBS; OCGS; ICF: Rockville, MA, USA, 2016. [Google Scholar]
- Yargawa, J.; Leonarde-Be, J. Male involvement and maternal health outcomes: Systematic review and meta-analysis. J. Epidemiol. Community Health 2015, 69, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Community Development, Gender and Children. Tanzania District Health Information System 2 (TDHIS2); Ministry of Health, Community Development, Gender and Children: Dar es Salaam, Tanzania, 2018. [Google Scholar]
- Mtae, H.G. Fertility preferences in Tanzania. In Assessment of Determinants of Couples’ Decisions on Fertility Preferences in Kishapu and Mvomero District, Tanzania; The Open University Of Tanzania: Dar es Salaam, Tanzania, 2018. [Google Scholar]
- Segele, A.J.; Mbonile, M.J. The Role of Sexual Reproductive Health Awareness in Reducing HIV Infections among Youth in Kibaha District, Tanzania. J. Geogr. Assoc. Tanzan. 2020, 27, 39–62. [Google Scholar]
- Chodota, V.E.; Mbonile, M.J.; Mwamfupe, A. Assessment of Factors Influencing Maternal High-risk Births in Njombe District, Tanzania. J. Geogr. Assoc. Tanzan. 2020, 40, 157–177. [Google Scholar]
- Shongwe, P.; Ntuli, B.; Madiba, S. Assessing the acceptability of vasectomy as a family planning option: A qualitative study with men in the kingdom of Eswatini. Int. J. Environ. Res. Public Health 2019, 16, 5158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO); United States Agency for International Development (USAID). Repositioning Family Planning: Guidelines for Advocacy Action; World Health Organization (WHO): Geneva, Switzerland; United States Agency for International Development (USAID): Washington, DC, USA, 2008; pp. 10–64. [Google Scholar]
- Kassa, M.; Alemu, A.A.; Gedefaw, M. Level of male involvement and associated factors in family planning services utilization among married men in Debremarkos town, Northwest Ethiopia. BMC Int. Health Hum. Rights 2014, 14, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wondim, G.; Degu, G.; Teka, Y.; Diress, G. Male involvement in family planning utilization and associated factors in Womberma District, Northern Ethiopia: Community-based cross-sectional study. Open Access J. Contracept. 2020, 11, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Amuzie, C.I.; Nwamoh, U.N.; Ukegbu, A.; Umeokonkwo, C.D.; Azuogu, B.N.; Agbo, U.O.; Balogun, M.S. Determinants of male involvement in family planning services in Abia State, Southeast Nigeria. Contracept. Reprod. Med. 2022, 7, 15. [Google Scholar] [CrossRef]
- National Statistical Office (NSO) [Malawi]; ICF. Malawi Demographic and Health Survey 2015–2016; NSO: Zomba, Malawi; ICF: Rockville, MD, USA, 2017. [Google Scholar]
- Tanzania Demographic and Health Survey (2015–2016). 2015–2016 Tanzania Demographic and Health Survey; ICF International, Ministry of Health (Zanzibar), Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDEC) (Tanzania), National Bureau of Statistics (Tanzania), Office of the Chief Government Statistician (OCGS) (Zanzibar); ICF International: Fairfax, WV, USA, 2016. [Google Scholar]
- The Demographic Health Survey (DHS) Program (2022). MeasureDHS. Available online: https://www.dhsprogram.com/ (accessed on 27 December 2022).
- Casey, S.E.; Gallagher, M.C.; Kakesa, J.; Kalyanpur, A.; Muselemu, J.B.; Rafanoharana, R.V.; Spilotros, N. Contraceptive use among adolescent and young women in North and South Kivu, Democratic Republic of the Congo: A cross-sectional population-based survey. PLoS Med. 2020, 17, e1003086. [Google Scholar] [CrossRef]
- Wiafe, E. Male Involvement in Family Planning in the Sunyani Municipality. MPH Dissertation, University of Ghana, Ghana, Accra, 2015. [Google Scholar]
- Koffi, T.B.; Weidert, K.; Bitasse, E.O.; Mensah, M.A.E.; Emina, J.; Mensah, S.; Bongiovanni, A.; Prata, N. Engaging men in family planning: Perspectives from married men in Lomé, Togo. Glob. Health Sci. Pract. 2018, 6, 316–327. [Google Scholar] [CrossRef] [Green Version]
- Demissie, G.D.; Akalu, Y.; Gelagay, A.A.; Alemnew, W.; Yeshaw, Y. Factors associated with decision-making power of married women to use family planning in sub-Saharan Africa: A multilevel analysis of demographic health surveys. BMC Public Health 2022, 22, 837. [Google Scholar] [CrossRef]
- Kamal, M.M.; Islam, S.; Alam, M.S.; Hassan Enamol, A.B.M. Determinants of male involvement in family planning and reproductive health in Bangladesh. Am. J. Hum. Ecol. 2013, 2, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Gueye, A.; Speizer, I.S.; Corroon, M.; Okigbo, C.C. Belief in Family Planning Myths at the Individual and Community Levels and Modern Contraceptive Use in Urban Africa. Int. Perspect. Sex. Reprod. Health 2015, 41, 191–199. [Google Scholar] [CrossRef]
- Iribhogbe, O.I.; Akpamu, U.; Nwaopara, A.O.; Osifo, U.C.; Otamere, H.O.; Okhiai, O.; Nwoke, E.O. Contraceptive choice amongst married men in Ekpoma, Nigeria. Afr. J. Biomed. Res. 2011, 3, 213–218. [Google Scholar]
- Rekha, T.; Unnikrishnan, B.; Mithra, P.P.; Kumar, N.; Holla, R.; Raina, V.; Hashim, H.; Singh, P. Married men’s involvement in family planning—A study from coastal Southern India. J. Clin. Diagn. Res. 2015, 9, LCO4–LCO7. [Google Scholar]
- Dougherty, A.; Kayongo, A.; Deans, S.; Mundaka, J.; Nassali, F.; Sewanyana, J.; Migadde, E.; Kiyemba, R.; Katali, E.; Holcombe, S.J.; et al. Knowledge and use of family planning among men in rural Uganda. BMC Public Health 2018, 18, 1294. [Google Scholar] [CrossRef]
- Butto, D.; Mburu, S. Factors associated with male involvement in family planning in West Pakot County, Kenya. Univ. J Public Health 2015, 3, 160–168. [Google Scholar] [CrossRef] [Green Version]
- Kassa, B.G.; Tenaw, L.A.; Ayele, A.D.; Tiruneh, G.A. Prevalence and determinants of the involvement of married men in family planning services in Ethiopia: A systematic review and meta-analysis. Women’s Health 2022, 18, 17455057221099083. [Google Scholar] [CrossRef]
- Ijadunola, M.Y.; Abiona, T.C.; Ijadunola, K.T.; Afolabi, O.T.; Esimai, O.A.; OlaOlurun, F.M. Male involvement in family planning decision—Making in Ile-Ife, Osun State, Nigeria. Afr. J. Reprod. Health 2010, 14, 43–50. [Google Scholar] [PubMed]
- Dennis, B.; Factors, M.S. Associated with male involvement in FP in west Pokot County, Kenya Universal. J. Public Health 2015, 2, 12547. [Google Scholar]
- Egbe, T.O.; Ketchen, S.A.; Egbe, E.-N.; Ekane, G.E.H.; Belley-Priso, E. Risk Factors and Barriers to Male Involvement in the Choice of Family Planning Methods in the Buea Health District, South West Region, Cameroon: A cross-sectional study in a Semi-Urban area. Women Health Open J. 2016, 1, 82–90. [Google Scholar] [CrossRef]
- Yeshareg, W.; Zelalem, A.; Liles, S. The current states of male involvement in family planning and factors correlated with among male factory workers in Bahir Dar City, Ethiopia. Am. J. Public Health Res. 2014, 2, 232–238. [Google Scholar]
- Kok, M.; Tolani, M.; Mtonga, W.; Salamba, T.; Mwabungulu, T.; Munthali, A.; Smet, E.; Chinsakaso, B. Enabling and hindering factors of health surveillance assistants’ roles in the provision of contraceptive services in Mangochi, Malawi. Reprod. Health 2020, 17, 57. [Google Scholar] [CrossRef] [Green Version]
- Apanga, P.A.; Adam, M.A. Factors influencing the uptake of family planning services in the Talensi District, Ghana. Pan Afr. Med. J. 2015, 20, 10. [Google Scholar] [CrossRef]
- Eliason, S.; Baiden, F.; Quansah-Asare, G.; Graham-Hayfron, Y.; Bonsu, D.; Phillips, J.; Awusabo-Asare, K. Factors influencing the intention of women in rural Ghana to adopt postpartum family planning. Reprod. Health 2013, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Shahjahan, M.; Kabir, M. Why males in Bangladesh do not participate in reproductive health: Lessons learned from focus group discussions. Int. Q. Community Health Educ. 2006, 26, 45–59. [Google Scholar] [CrossRef]
- Ardiansyah, B. Effect of Mass Media on Family Planning Choices in Indonesia. In MPA/MPP/MPFM Capstone Projects; James W. Martin School of Public Policy and Administration, University of Kentucky: Lexington, KY, USA, 2016; p. 243. [Google Scholar]
- Chakraborty, N.M.; Sprockett, A. Use of family planning and child health services in the private sector: An equity analysis of 12 DHS surveys. Int. J. Equity Health 2018, 17, 50. [Google Scholar] [CrossRef] [Green Version]
- Anbesu, E.W.; Aychiluhm, S.B.; Kahsay, Z.H. Male involvement in family planning use and its determinants in Ethiopia: A systematic review and meta-analysis protocol. Syst. Rev. 2022, 11, 19. [Google Scholar] [CrossRef]
- Ahn, J.; Briers, G.; Baker, M.; Price, E.; Strong, R.; Piña, M.; Zickafoose, A.; Lu, P. Radio Communications on Family Planning: Case of West Africa. Int. J. Environ. Res. Public Health 2022, 19, 4577. [Google Scholar] [CrossRef]
- Corey, J.; Schwandt, H.; Boulware, A.; Herrera, A.; Hudler, E.; Imbabazi, C.; King, I.; Linus, J.; Manzi, I.; Merrit, M.; et al. Family planning demand generation in Rwanda: Government efforts at the national and community level impact interpersonal communication and family norms. PLoS ONE 2022, 17, e0266520. [Google Scholar] [CrossRef] [PubMed]
- Adelaida, T.; Anja, V.; Chris, M.; Daniel, V.S.; Deanna, B.; Schlackl, J.; Marulanda, J.; DeVries, K.; Martin, V.; Feek, W.; et al. The Impact of a Male Motivation Campaign on FP Attitudes and Practices in Guinea; Blake, M., Babalola, S., Eds.; The Communication Initiative: Victoria, BC, Canada; Johns Hopkins Bloomberg School of Public Health Center for Communications Programs: Baltimore, MD, USA, 2009. [Google Scholar]
- Maharaj, P. Promoting Male Involvement in Reproductive Health. Agenda Empower. Women Gend. Equity 2000, 44, 37–47. [Google Scholar] [CrossRef]
- Mutumba, M. Mass media influences on family planning knowledge, attitudes and method choice among sexually active men in sub-Saharan Africa. PLoS ONE 2022, 17, e0261068. [Google Scholar] [CrossRef]
- Akokuwebe, M.E.; Omololu, F.; Sanda, K.A.; Adekola, F. Influence of Social Media on Academic Performance of Undergraduates in a Public University-Nigeria; The Concise Demography of Nigeria; Nwokocha, E.E., Fayehun, O., Eds.; BumbleBee Publishing: Ibadan, Nigeria, 2019; pp. 312–329. [Google Scholar]
- Akokuwebe, M.E.; Oluwawole, A.O. Factors influencing acceptability of family planning among women in rural communities in Ife central local government area, Osun State. Ibadan J. Soc. Sci. 2016, 14, 250–261. [Google Scholar]
- Akokuwebe, M.E.; Idemudia, E.S. Factors associated with choice of home birth as place of delivery among women of reproductive age in South Africa. Afr. J. Reprod. Health 2023, 27, 22–40. [Google Scholar]
- Aslam, S.K.; Zaheer, S.; Qureshi, M.S.; Aslam, S.N.; Shafique, K. Socio-economic disparities in use of family planning methods among Pakistani women: Findings from Pakistan Demographic and Health Surveys. PLoS ONE 2016, 11, e0153313. [Google Scholar] [CrossRef]
- Ekholuenetale, M.; Owobi, O.U.; Shishi, B.T. Socio-economic position in modern contraceptive uptake and fertility rate among women of childbearing age in 37 sub-Saharan countries. World 2022, 3, 858–875. [Google Scholar] [CrossRef]
- Sundararajan, R.; Yoder, L.M.; Kihunrwa, A.; Aristide, C.; Kalluvya, S.E.; Downs, D.J.; Mwakisole, A.H.; Downs, J.A. How gender and religion impact uptake of family planning: Results from a qualitative study in Northwestern Tanzania. BMC Women’s Health 2019, 19, 99. [Google Scholar] [CrossRef] [Green Version]
- Mejía-Guevara, I.; Cislaghi, B.; Darmstadt, G.L. Men’s Attitude Towards Contraception and Sexuality, Women’s Empowerment, and Demand Satisfied for Family Planning in India. Front. Sociol. 2021, 6, 689980. [Google Scholar] [CrossRef] [PubMed]
- Mulatu, T.; Sintayehu, Y.; Dessie, Y.; Dheresa, M. Male involvement in family planning use and associated factors among currently married men in rural Eastern Ethiopia. SAGE Open Med. 2022, 10, 1–7. [Google Scholar] [CrossRef]
- Docklova, B.; Lau, K.; Barclay, H.; Marshall, A. From Choice, a World of Possibilities: Sustainable Development Goals and Family Planning 2020; International Planned Parenthood Federation (IPPF): London, UK, 2020; pp. 1–12. [Google Scholar]
- Jurczynska, K.; Moreland, S.; Sacher, S.; Bispo, S.; Corpuz, K. Modeling the Effects of Family Planning on the Sustainable Development Goals: Family Planning-Sustainable Development Goals Model Methodology and User’s Guide; Palladium, Health Policy Plus: Washington, DC, USA, 2018. [Google Scholar]
- Starbird, E.; Norton, M.; Marcus, R. Investing in family planning: Key to achieving the sustainable development goals. Glob. Health Sci. Pract. 2016, 4, 191–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chereni, A.; Nyathi, N.; Mbizo, J. Male partner involvement in health interventions: A systematic review of best practices in Sub-Saharan Africa. J. Pract. Teach. Learn. 2020, 19, 87–113. [Google Scholar] [CrossRef]
- Ogu, R.N.; Agholor, K.N.; Okonofua, F.E. Engendering the Attainment of the SDG-3 in Africa: Overcoming the Socio-Cultural Factors Contributing to Maternal Mortality. Afr. J. Reprod. Health 2016, 20, 62. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable Name | Definition (Measurement) |
|---|---|
| Age | Categorized as: 15–24, 25–34, 35–44, and 45–54 years |
| Place of residence | Categorized as: “rural” and “urban” |
| Education | Categorized as: “no education”, “primary education”, and “secondary/higher” |
| Wealth status | Categorized as: “poor”, “middle” and “rich” |
| Religion | Categorized as: “Christian”, “Muslim”, and “Traditional” |
| Marital status | Categorized as: “never married”, “married/cohabiting”, “widowed” and “divorced/separated” |
| Occupation | Categorized as: “not working” and “working” |
| Access to media information | Categorized as: “no” and “yes” |
| Contraceptive knowledge | Categorized as: “poor” and “good” |
| Sex of household head | Categorized as: “male-headed” and “female-headed” |
| Socio-Demographic Factors | Malawi, n = 7478 | Tanzania = 3514 |
|---|---|---|
| Age (in years) | ||
| 15–24 | 3226 (43.1%) | 1556 (44.3%) |
| 25–34 | 1975 (26.4%) | 900 (25.6%) |
| 35–44 | 1485 (19.9%) | 762 (21.7%) |
| 45–54 | 792 (10.6%) | 296 (8.4%) |
| Place of residence | ||
| Urban | 1661 (22.2%) | 1057 (30.1%) |
| Rural | 5817 (77.8%) | 2457 (69.9%) |
| Educational attainment | ||
| No education | 399 (5.3%) | 279 (7.9%) |
| Primary | 4252 (56.9%) | 2175 (61.9%) |
| Secondary/higher | 2827 (37.8%) | 1060 (30.2%) |
| Wealth status | ||
| Poor | 2365 (31.6%) | 1162 (33.1%) |
| Middle | 1443 (19.3%) | 688 (19.6%) |
| Rich | 3670 (49.1%) | 1664 (47.3%) |
| Religion | – | |
| Christian | 6560 (87.7%) | – |
| Muslim | 726 (9.7%) | – |
| Traditional | 192 (2.6%) | – |
| Marital status | ||
| Never married | 2932 (39.2%) | 1580 (45.0%) |
| Married/cohabiting | 4284 (57.3%) | 1768 (50.3%) |
| Widowed | 36 (0.5%) | 17 (0.5%) |
| Divorced/Separated | 226 (3.0%) | 149 (4.2%) |
| Occupational status | ||
| Not working | 1089 (14.6%) | 408 (11.6%) |
| Working | 6389 (85.4%) | 3106 (88.4%) |
| Access to media information | ||
| No | 1677 (22.4%) | 440 (12.5%) |
| Yes | 5801 (77.6%) | 3074 (87.5%) |
| Contraceptive knowledge | ||
| Poor | 40 (0.5%) | 76 (2.2%) |
| Good | 7438 (99.5%) | 3438 (97.8%) |
| Sex of household head | ||
| Male head | 6316 (84.5%) | 3029 (86.2%) |
| Female head | 1162 (15.5%) | 485 (13.8%) |
| Socio-Demographic Factors | Malawi | Tanzania | ||
|---|---|---|---|---|
| No | Yes | No | Yes | |
| Age (in years) | p = 0.000; χ2 = 149.1174 * | p = 0.000; χ2 = 95.7591 * | ||
| 15–24 | 1769 (54.8) | 1457 (45.2) | 1265 (81.3) | 291 (18.7) |
| 25–34 | 785 (39.8) | 1190 (60.3) | 599 (66.6) | 301 (33.4) |
| 35–44 | 597 (40.2) | 888 (59.8) | 499 (65.5) | 263 (34.5) |
| 45–54 | 364 (46.0) | 428 (54.0) | 215 (72.6) | 81 (27.4) |
| Place of residence | p = 0.065; χ2 = 4.4266 | p = 0.000; χ2 = 26.1499 * | ||
| Urban | 743 (44.7) | 918 (55.3) | 714 (67.6) | 343 (32.5) |
| Rural | 2772 (47.7) | 3045 (52.4) | 1864 (75.9) | 593 (24.1) |
| Educational attainment | p = 0.000; χ2 = 62.4618 * | p = 0.102; χ2 = 21.1030 | ||
| No education | 212 (53.1) | 187 (46.9) | 235 (84.2) | 44 (15.8) |
| Primary | 2138 (50.3) | 2114 (49.7) | 1595 (73.3) | 580 (26.7) |
| Secondary/higher | 1165 (41.2) | 1662 (58.8) | 748 (70.6) | 312 (29.4) |
| Wealth status | p = 0.404; χ2 = 11.2283 | p = 0.005; χ2 = 34.0326 * | ||
| Poor | 1165 (49.3) | 1200 (50.7) | 922 (79.4) | 240 (20.7) |
| Middle | 696 (48.2) | 747 (51.8) | 499 (72.5) | 189 (27.5) |
| Rich | 1654 (45.1) | 2016 (54.9) | 1157 (69.53) | 507 (30.5) |
| Religion | p = 0.002; χ2 = 12.1411 * | - | ||
| Christian | 3036 (46.3) | 3524 (53.7) | - | - |
| Muslim | 373 (51.4) | 353 (48.6) | - | - |
| Traditional | 106 (55.2) | 86 (44.8) | - | - |
| Marital status | p = 0.001; χ2 = 111.6213 * | p = 0.005; χ2 = 55.7393 * | ||
| Never married | 1592 (54.3) | 1340 (45.7) | 1247 (78.9) | 333 (21.1) |
| Married/cohabiting | 1828 (42.7) | 2456 (57.3) | 1234 (69.8) | 534 (30.2) |
| Widowed | 19 (52.8) | 17 (47.2) | 9 (52.9) | 8 (47.1) |
| Divorced/Separated | 76 (33.6) | 150 (66.4) | 88 (59.1) | 61 (40.9) |
| Occupational status | p = 0.080; χ2 = 178.0138 | p = 0.005; χ2 = 48.8549 * | ||
| Not working | 715 (65.7) | 374 (34.3) | 358 (87.8) | 50 (12.25) |
| Working | 2800 (43.8) | 3589 (56.2) | 2220 (71.5) | 886 (28.5) |
| Access to media information | p = 0.001; χ2 = 29.4754 * | p = 0.902; χ2 = 56.5174 | ||
| No | 886 (52.8) | 791 (47.2) | 388 (88.2) | 52 (11.8) |
| Yes | 2629 (45.3) | 3172 (54.7) | 2190 (71.2) | 884 (28.8) |
| Contraceptive knowledge | p = 0.000; χ2 = 45.3407 * | p = 0.006; χ2 = 28.2035 | ||
| Poor | 40 (100.0) | 00 (100.0) | 76 (100.0) | 00 (100.0) |
| Good | 3475 (46.7) | 3963 (53.3) | 2502 (72.8) | 936 (27.3) |
| Sex of household head | p = 0.004; χ2 = 13.1997 * | p = 0.057; χ2 = 3.6154 | ||
| Male | 2912 (46.1) | 3404 (53.9) | 2205 (72.8) | 824 (27.2) |
| Female | 603 (51.9) | 559 (48.1) | 373 (76.9) | 112 (23.1) |
| Sociodemographic Factors | Malawi | Tanzania | ||
|---|---|---|---|---|
| Age (in years) | UOR | AOR | UOR | AOR |
| 15–24 | RC | RC | RC | RC |
| 25–34 | 1.47 (1.26–1.72) | 1.84 (1.64–2.06) | 1.89 (1.47–2.44) | 2.18 (1.81–2.64) |
| 35–44 | 1.47 (1.24–1.75) * | 1.81 (1.59–2.05) ** | 2.00 (1.50–2.67) | 2.29 (1.88–2.79) |
| 45–54 | 1.25 (1.03–1.53) * | 1.43 (1.22–1.67) ** | 1.49 (1.04–2.13) | 1.64 (1.23–2.18) |
| Place of residence | ||||
| Urban | RC | RC | RC | RC |
| Rural | 0.98 (0.86–1.12) | 0.89 (0.80–0.99) | 0.79 (0.65–0.96) * | 0.66 (0.57–0.78) * |
| Educational level | ||||
| No education | RC | RC | RC | RC |
| Primary | 1.25 (1.01–1.55) | 1.12 (0.91–1.38) | 1.90 (1.34–2.68) *** | 1.94 (1.39–2.72) ** |
| Secondary/higher | 1.72 (1.37–2.15) ** | 1.62 (1.31–1.99) *** | 2.35 (1.61–3.42) | 2.23 (1.57–3.16) |
| Wealth status | ||||
| Poor | RC | RC | RC | RC |
| Middle | 1.01 (0.89–1.16) | 1.04 (0.91–1.19) | 1.26 (1.00–1.58) *** | 1.46 (1.17–1.81) *** |
| Rich | 1.06 (0.93–1.20) ** | 1.18 (1.07–1.31) ** | 1.17 (0.94–1.47) | 1.68 (1.41–2.01) |
| Religion | ||||
| Christian | RC | RC | RC | RC |
| Muslim | 0.86 (0.74–1.01) * | 0.82 (0.70–0.95) * | ||
| Traditional | 0.74 (0.55–1.00) * | 0.70 (0.52–0.93) * | ||
| Marital status | ||||
| Never married | RC | RC | RC | RC |
| Married/cohabiting | 1.04 (0.89–1.22) | 1.60 (1.45–1.75) | 0.94 (0.73–1.21) * | 1.62 (1.38–1.90) * |
| Widowed | 0.74 (0.38–1.47) | 1.06 (0.55–2.05) | 1.99 (0.71–5.62) | 3.33 (1.27–8.70) |
| Divorced/Separated | 1.56 (1.15–2.13) | 2.34 (1.76–3.12) | 1.60 (1.08–2.39) | 2.60 (1.83–3.68) |
| Occupational status | ||||
| Not working | RC | RC | RC | RC |
| Working | 2.07 (1.78–2.40) | 2.45 (2.14–2.80) | 2.33 (1.67–3.26) ** | 2.86 (2.10–3.88) ** |
| Access to media information | ||||
| No | RC | RC | RC | RC |
| Yes | 1.18 (1.06–1.33) * | 1.35 (1.21–1.51) * | 2.45 (1.79–3.33) | 3.01 (2.23–4.06) |
| Sex of household head | ||||
| Male | RC | RC | RC | RC |
| Female | 1.02 (0.89–1.17) ** | 1.79 (1.70–1.90) * | 0.91 (0.71–1.15) ** | 0.80 (0.64–1.01) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osuafor, G.N.; Akokuwebe, M.E.; Idemudia, E.S. Male Involvement in Family Planning Decisions in Malawi and Tanzania: What Are the Determinants? Int. J. Environ. Res. Public Health 2023, 20, 5053. https://doi.org/10.3390/ijerph20065053
Osuafor GN, Akokuwebe ME, Idemudia ES. Male Involvement in Family Planning Decisions in Malawi and Tanzania: What Are the Determinants? International Journal of Environmental Research and Public Health. 2023; 20(6):5053. https://doi.org/10.3390/ijerph20065053
Chicago/Turabian StyleOsuafor, Godswill Nwabuisi, Monica Ewomazino Akokuwebe, and Erhabor Sunday Idemudia. 2023. "Male Involvement in Family Planning Decisions in Malawi and Tanzania: What Are the Determinants?" International Journal of Environmental Research and Public Health 20, no. 6: 5053. https://doi.org/10.3390/ijerph20065053