
Inflammatory and Prothrombotic Biomarkers Contribute to the Persistence of Sequelae in Recovered COVID-19 Patients
 ,
,
Abstract
:1. Introduction
2. Results
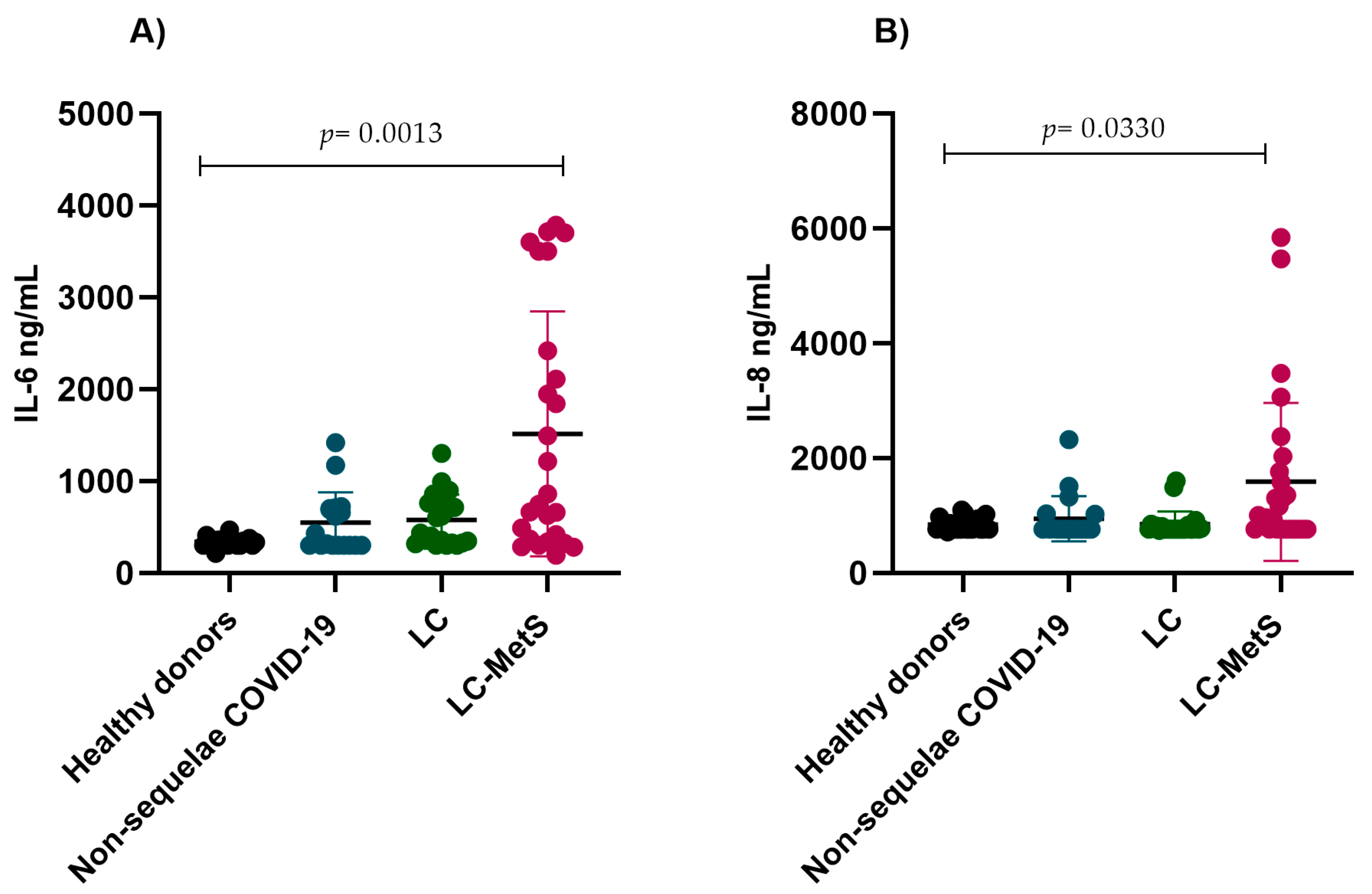
2.1. Immunothrombotic Biomarkers
2.2. Von Willebrand Factor
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Samples
4.3. Immunothrombotic Biomarkers
4.4. Von Willebrand Factor
4.5. Statistical Analysis
4.6. Ethics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Chen, B.; Julg, B.; Mohandas, S.; Bradfute, S.B.; RECOVER Mechanistic Pathways Task Force. Viral persistence, reactivation, and mechanisms of long COVID. eLife 2023, 12, e86015. [Google Scholar] [CrossRef]
- Lai, C.C.; Hsu, C.K.; Yen, M.Y.; Lee, P.I.; Ko, W.C.; Hsueh, P.R. Long COVID: An inevitable sequela of SARS-CoV-2 infection. J. Microbiol. Immunol. Infect. 2023, 56, 1–9. [Google Scholar] [CrossRef]
- Phetsouphanh, C.; Darley, D.R.; Wilson, D.B.; Howe, A.; Munier, C.M.L.; Patel, S.K.; Juno, J.A.; Burrell, L.M.; Kent, S.J.; Dore, G.J.; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat. Immunol. 2022, 23, 210–216. [Google Scholar] [CrossRef]
- Pintos-Pascual, I.; Moreno-Torres, V.; Ibánez-Estéllez, F.; Corrales-Rodriguez, P.; Treviño, A.; Corpas, M.; Corral, O.; Soriano, V.; de Mendoza, C. Is SARS-CoV-2 the only cause of long-COVID? AIDS Rev. 2022, 24, 183–196. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C. Long COVID: Current definition. Infection 2022, 50, 285–286. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Cabrera Martimbianco, A.L.; Pacheco, R.L.; Bagattini, Â.M.; Riera, R. Frequency, signs and symptoms, and criteria adopted for long COVID-19: A systematic review. Int. J. Clin. Pract. 2021, 75, e14357. [Google Scholar] [CrossRef]
- Healey, Q.; Sheikh, A.; Daines, L.; Vasileiou, E. Symptoms and signs of long COVID: A rapid review and meta-analysis. J. Glob. Health 2022, 12, 05014. [Google Scholar] [CrossRef]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Barbouzas, A.E.; Malli, F.; Daniil, Z.; Gourgoulianis, K. Long-Term Impact of COVID-19 Pandemic in Sleep Quality and Lifestyle in Young Adults. Int. J. Environ. Res. Public Health 2022, 19, 12333. [Google Scholar] [CrossRef]
- Astin, R.; Banerjee, A.; Baker, M.R.; Dani, M.; Ford, E.; Hull, J.H.; Lim, P.B.; McNarry, M.; Morten, K.; O’Sullivan, O.; et al. Long COVID: Mechanisms, risk factors and recovery. Exp. Physiol. 2023, 108, 12–27. [Google Scholar] [CrossRef]
- Zhang, H.P.; Sun, Y.L.; Wang, Y.F.; Yazici, D.; Azkur, D.; Ogulur, I.; Azkur, A.K.; Yang, Z.W.; Chen, X.X.; Zhang, A.Z.; et al. Recent developments in the immunopathology of COVID-19. Allergy 2023, 78, 369–388. [Google Scholar] [CrossRef]
- Altmann, D.M.; Whettlock, E.M.; Liu, S.; Arachchillage, D.J.; Boyton, R.J. The immunology of long COVID. Nat. Rev. Immunol. 2023, 23, 618–634. [Google Scholar] [CrossRef]
- Turner, S.; Khan, M.A.; Putrino, D.; Woodcock, A.; Kell, D.B.; Pretorius, E. Long COVID: Pathophysiological factors and abnormalities of coagulation. Trends Endocrinol. Metab. TEM 2023, 34, 321–344. [Google Scholar] [CrossRef]
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, A. The immunology and immunopathology of COVID-19. Science 2022, 375, 1122–1127. [Google Scholar] [CrossRef]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef]
- Nicolai, L.; Kaiser, R.; Stark, K. Thromboinflammation in long COVID-the elusive key to postinfection sequelae? J. Thromb. Haemost. JTH 2023, 21, 2020–2031. [Google Scholar] [CrossRef]
- Martins-Gonçalves, R.; Hottz, E.D.; Bozza, P.T. Acute to post-acute COVID-19 thromboinflammation persistence: Mechanisms and potential consequences. Curr. Res. Immunol. 2023, 4, 100058. [Google Scholar] [CrossRef]
- Jing, H.; Wu, X.; Xiang, M.; Liu, L.; Novakovic, V.A.; Shi, J. Pathophysiological mechanisms of thrombosis in acute and long COVID-19. Front. Immunol. 2022, 13, 992384. [Google Scholar] [CrossRef]
- Fogarty, H.; Ward, S.E.; Townsend, L.; Karampini, E.; Elliott, S.; Conlon, N.; Dunne, J.; Kiersey, R.; Naughton, A.; Gardiner, M.; et al. Sustained VWF-ADAMTS-13 axis imbalance and endotheliopathy in long COVID syndrome is related to immune dysfunction. J. Thromb. Haemost. JTH 2022, 20, 2429–2438. [Google Scholar] [CrossRef]
- Zanini, G.; Selleri, V.; Roncati, L.; Coppi, F.; Nasi, M.; Farinetti, A.; Manenti, A.; Pinti, M.; Mattioli, A.V. Vascular “Long COVID”: A New Vessel Disease? Angiology 2024, 75, 8–14. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Cozma, D.; Kamel, M.; Hamad, M.; Mohammad, M.G.; Khan, N.A.; Saber, M.M.; Semreen, M.H.; Steenblock, C. Long-COVID, Metabolic and Endocrine Disease. Horm. Metab. Res. 2022, 54, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, A.A.; Kathuria, A.; Al Mahmeed, W.; Al-Rasadi, K.; Al-Alawi, K.; Banach, M.; Banerjee, Y.; Ceriello, A.; Cesur, M.; Cosentino, F.; et al. Post-COVID syndrome, inflammation, and diabetes. J. Diabetes Its Complicat. 2022, 36, 108336. [Google Scholar] [CrossRef] [PubMed]
- Ruilope, L.M.; Nunes Filho, A.C.B.; Nadruz, W., Jr.; Rodríguez Rosales, F.F.; Verdejo-Paris, J. Obesity and hypertension in Latin America: Current perspectives. Hipertens. Y Riesgo Vasc. 2018, 35, 70–76. [Google Scholar] [CrossRef]
- Lopez-Castaneda, S.; García-Larragoiti, N.; Cano-Mendez, A.; Blancas-Ayala, K.; Damian-Vázquez, G.; Perez-Medina, A.I.; Chora-Hernández, L.D.; Arean-Martínez, C.; Viveros-Sandoval, M.E. Inflammatory and Prothrombotic Biomarkers Associated With the Severity of COVID-19 Infection. Clin. Appl. Thromb. Hemost. 2021, 27, 1076029621999099. [Google Scholar] [CrossRef] [PubMed]
- Yin, K.; Peluso, M.J.; Luo, X.; Thomas, R.; Shin, M.G.; Neidleman, J.; Andrew, A.; Young, K.; Ma, T.; Hoh, R.; et al. Long COVID manifests with T cell dysregulation, inflammation, and an uncoordinated adaptive immune response to SARS-CoV-2. bioRxiv 2023, 4, 527892. [Google Scholar] [CrossRef]
- Lehmann, A.; Prosch, H.; Zehetmayer, S.; Gysan, M.R.; Bernitzky, D.; Vonbank, K.; Idzko, M.; Gompelmann, D. Impact of persistent D-dimer elevation following recovery from COVID-19. PLoS ONE 2021, 16, e0258351. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Zhong, L.; Zhu, S.; Wang, Y.; Zheng, J.; Wang, S.; Zhang, J.; Huang, R. The P-selectin and PSGL-1 axis accelerates atherosclerosis via activation of dendritic cells by the TLR4 signaling pathway. Cell Death Dis. 2019, 10, 507. [Google Scholar] [CrossRef]
- Merten, M.; Thiagarajan, P. P-selectin in arterial thrombosis. Z Kardiol. 2004, 93, 855–863. [Google Scholar] [CrossRef]
- Zuo, Y.; Warnock, M.; Harbaugh, A.; Yalavarthi, S.; Gockman, K.; Zuo, M.; Madison, J.A.; Knight, J.S.; Kanthi, Y.; Lawrence, D.A. Plasma tissue plasminogen activator and plasminogen activator inhibitor-1 in hospitalized COVID-19 patients. Sci. Rep. 2021, 11, 1580. [Google Scholar] [CrossRef] [PubMed]
- Gorog, D.A.; Storey, R.F.; Gurbel, P.A.; Tantry, U.S.; Berger, J.S.; Chan, M.Y.; Duerschmied, D.; Smyth, S.S.; Parker, W.A.E.; Ajjan, R.A.; et al. Current and novel biomarkers of thrombotic risk in COVID-19: A Consensus Statement from the International COVID-19 Thrombosis Biomarkers Colloquium. Nat. Rev. Cardiol. 2022, 19, 475–495. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Healthy Donors (n = 23) | Non-Sequelae COVID-19 (n = 19) | LC (n = 21) | LC-MetS (n = 26) | p Value |
|---|---|---|---|---|---|
| Age (mean ± SD) | 25.4 ± 4.9 | 20.1 ± 2.4 | 21.7 ± 5.3 | 51 ± 15.1 | 0.007 |
| Female (%) | 70 | 84.2 | 61.9 | 53.8 | 0.185 |
| BMI (mean ± SD) | 24.9 ± 3.5 | 23.6 ± 3.1 | 21.9 ± 3.4 | 30.9 ± 1.8 | 0.081 |
| Vaccinated against SARS-CoV-2 (%) | N/A | 94.7 | 100 | 96.1 | 0.0605 |
| Pfizer | 84.2 | 85.9 | 50 | ||
| AstraZeneca | 10.5 | 4.7 | 30.8 | ||
| CanSino | 0 | 4.7 | 15.3 | ||
| Moderna | 0 | 4.7 | 0 | ||
| Non vaccinated | 5.3 | 0 | 3.9 |
| Characteristic | LC (n = 21) | LC-MetS (n = 26) | p Value |
|---|---|---|---|
| Headache | 38.0 | 38.4 | 0.99 |
| Tachycardia | 9.52 | 3.8 | 0.57 |
| Fever | 4.7 | 3.8 | 0.99 |
| Cough | 61.9 | 34.6 | 0.08 |
| Anxiety | 47.6 | 26.9 | 0.22 |
| Ageusia | 4.7 | 7.6 | 0.99 |
| Digestive problems | 4.7 | 3.8 | 0.99 |
| Fatigue | 14.2 | 7.6 | 0.64 |
| Anosmia | 33.3 | 19.2 | 0.32 |
| Myalgias | 9.5 | 42.3 | 0.02 |
| Sore throat | 4.7 | 0 | 0.44 |
| Low back pain | 14.2 | 30.7 | 0.30 |
| Arthralgia | 14.2 | 38.4 | 0.10 |
| Urticaria | 9.5 | 3.8 | 0.57 |
| Arrhythmia | 4.7 | 0 | 0.45 |
| Rhinorrhea | 4.76 | 11.54 | 0.61 |
| Sleep disorders | 19.05 | 34.62 | 0.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Larragoiti, N.; Cano-Mendez, A.; Jimenez-Vega, Y.; Trujillo, M.; Guzman-Cancino, P.; Ambriz-Murillo, Y.; Viveros-Sandoval, M.E. Inflammatory and Prothrombotic Biomarkers Contribute to the Persistence of Sequelae in Recovered COVID-19 Patients. Int. J. Mol. Sci. 2023, 24, 17468. https://doi.org/10.3390/ijms242417468
Garcia-Larragoiti N, Cano-Mendez A, Jimenez-Vega Y, Trujillo M, Guzman-Cancino P, Ambriz-Murillo Y, Viveros-Sandoval ME. Inflammatory and Prothrombotic Biomarkers Contribute to the Persistence of Sequelae in Recovered COVID-19 Patients. International Journal of Molecular Sciences. 2023; 24(24):17468. https://doi.org/10.3390/ijms242417468
Chicago/Turabian StyleGarcia-Larragoiti, Nallely, Alan Cano-Mendez, Yeny Jimenez-Vega, Mercedes Trujillo, Patricia Guzman-Cancino, Yesenia Ambriz-Murillo, and Martha Eva Viveros-Sandoval. 2023. "Inflammatory and Prothrombotic Biomarkers Contribute to the Persistence of Sequelae in Recovered COVID-19 Patients" International Journal of Molecular Sciences 24, no. 24: 17468. https://doi.org/10.3390/ijms242417468