
Chemotherapeutics Combined with Luminal Irritants: Effects on Small-Intestinal Mannitol Permeability and Villus Length in Rats

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Basal Intestinal Permeability
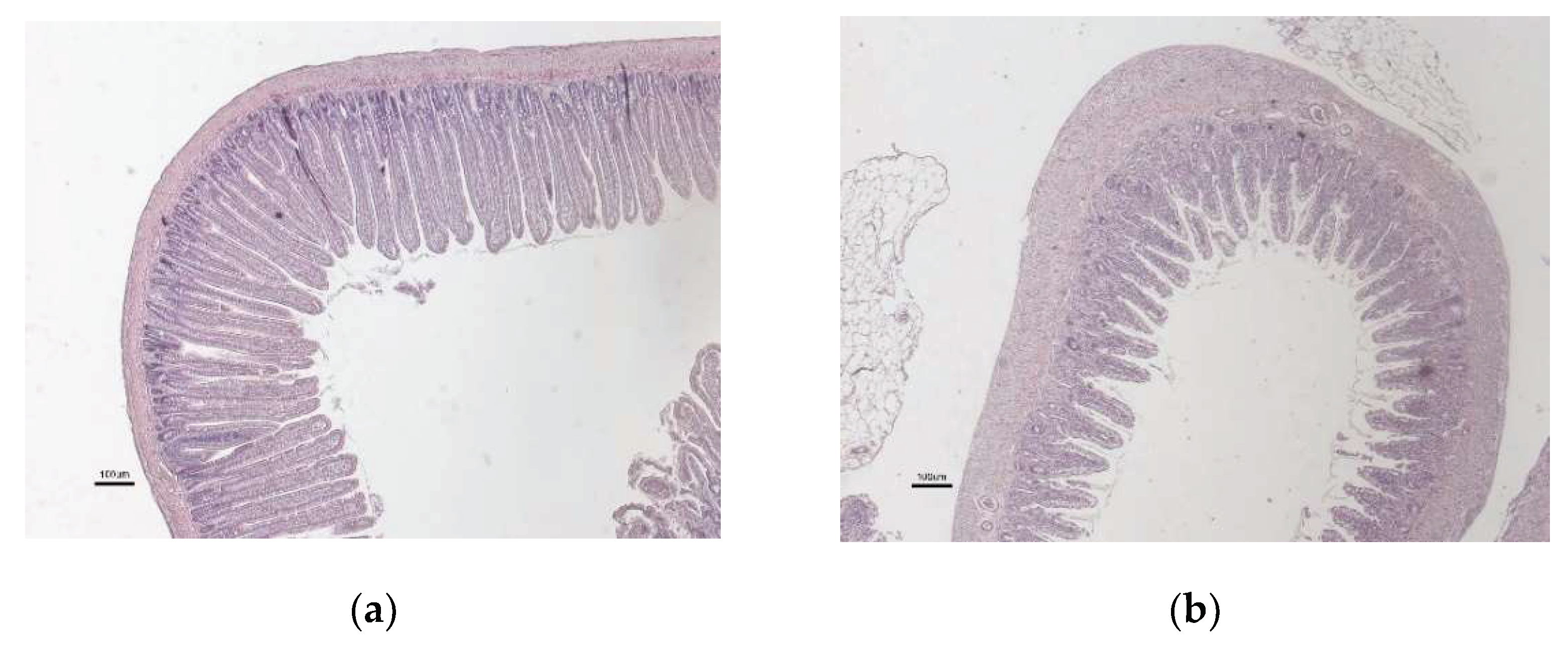
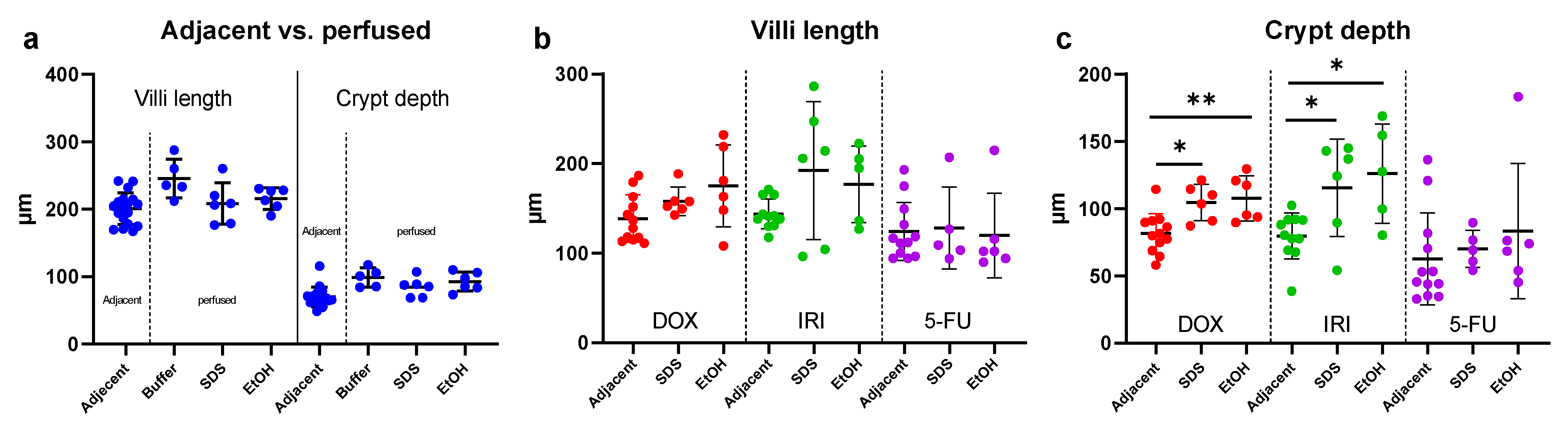
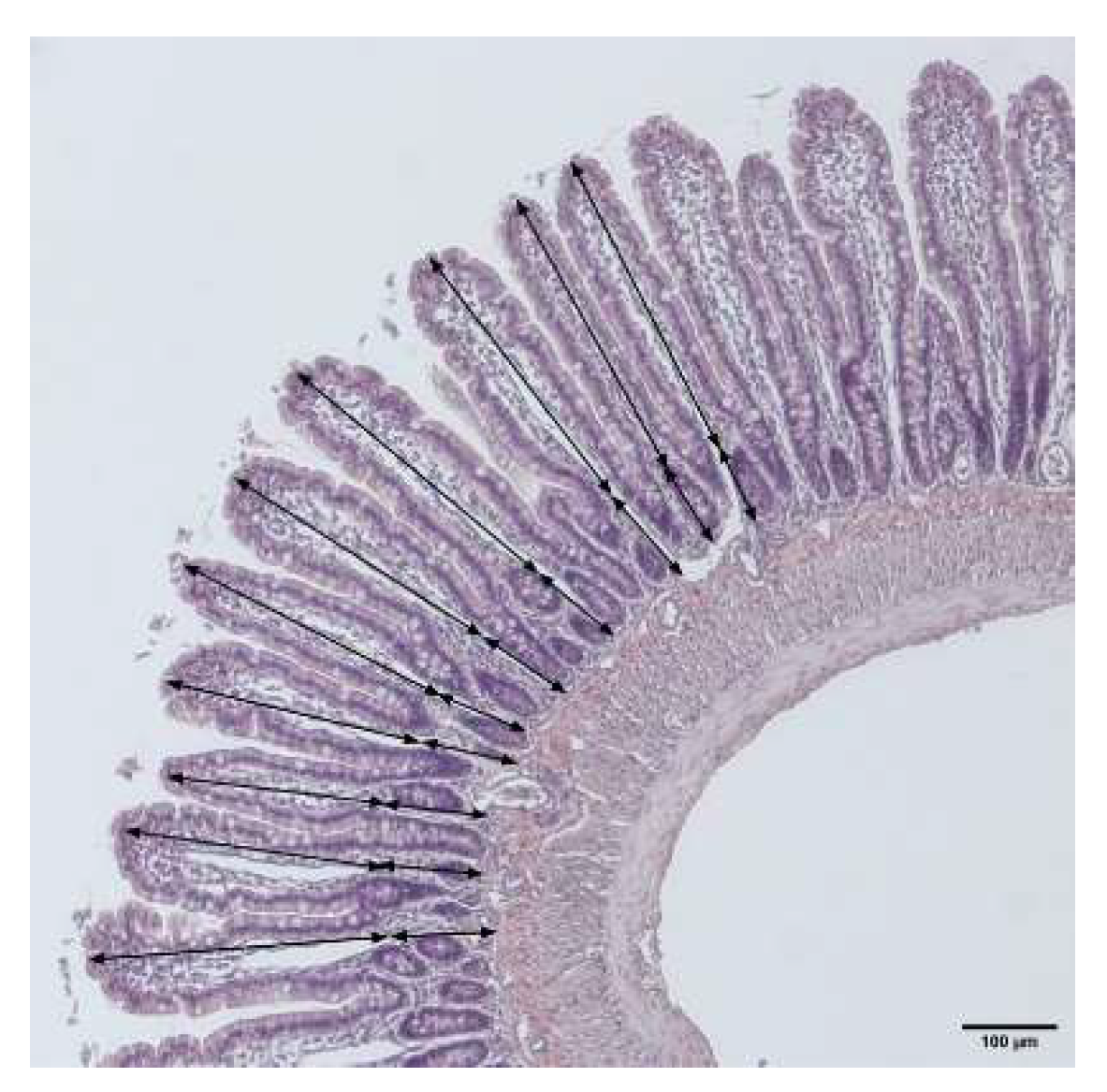
2.2. Villi Length and Crypt Depth
2.3. Correlation between Basal Intestinal Permeability and Villi Length
2.4. Effect of Luminal Irritants on Intestinal Permeability and Histology
3. Discussion
4. Materials and Methods
4.1. Chemicals
4.2. Study Formulations
4.3. Animals
4.4. Chemotherapy Dosing and Intestinal Perfusions
4.5. Determination of Blood-to-Lumen Jejunal 3H-Mannitol Clearance
4.6. Histology
4.7. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Weiderpass, E.; Soerjomataram, I. The ever-increasing importance of cancer as a leading cause of premature death worldwide. Cancer 2021, 127, 3029–3030. [Google Scholar] [CrossRef]
- Darwich, A.S.; Aslam, U.; Ashcroft, D.M.; Rostami-Hodjegan, A. Meta-analysis of the turnover of intestinal epithelia in preclinical animal species and humans. Drug Metab. Dispos. 2014, 42, 2016–2022. [Google Scholar] [CrossRef] [Green Version]
- Dahlgren, D.; Sjöblom, M.; Hellström, P.M.; Lennernäs, H. Chemotherapeutics-induced intestinal mucositis: Pathophysiology and potential treatment strategies. Front. Pharmacol. 2021, 12, 1020. [Google Scholar] [CrossRef]
- Keefe, D.M.; Elting, L.S.; Nguyen, H.T.; Grunberg, S.M.; Aprile, G.; Bonaventura, A.; Selva-Nayagam, S.; Barsevick, A.; Koczwara, B.; Sonis, S.T. Risk and outcomes of chemotherapy-induced diarrhea (CID) among patients with colorectal cancer receiving multi-cycle chemotherapy. Cancer Chemother. Pharmacol. 2014, 74, 675–680. [Google Scholar] [CrossRef]
- Helander, H.F.; Fändriks, L. Surface area of the digestive tract-revisited. Scand. J. Gastroenterol. 2014, 49, 681–689. [Google Scholar] [CrossRef]
- Avritscher, E.B.; Cooksley, C.D.; Elting, L.S. Scope and epidemiology of cancer therapy-induced oral and gastrointestinal mucositis. Proc. Semin. Oncol. Nurs. 2004, 20, 3–10. [Google Scholar] [CrossRef]
- Menzies, I.S. Absorption of intact oligosaccharide in health and disease. Biochem. Soc. Trans. 1974, 2, 1042–1047. [Google Scholar] [CrossRef] [Green Version]
- Vilela, E.; Torres, H.; Ferrari, M.; Lima, A.; Cunha, A. Gut permeability to lactulose and mannitol differs in treated Crohn’s disease and celiac disease patients and healthy subjects. Braz. J. Med. Biol. Res. 2008, 41, 1105–1109. [Google Scholar] [CrossRef] [Green Version]
- Bjarnason, I.; Macpherson, A.; Hollander, D. Intestinal permeability: An overview. Gastroenterology 1995, 108, 1566–1581. [Google Scholar] [CrossRef]
- Tooley, K.L.; Howarth, G.S.; Butler, R.N. Mucositis and non-invasive markers of small intestinal function. Cancer Biol. Ther. 2009, 8, 753–758. [Google Scholar] [CrossRef]
- Camilleri, M. Leaky gut: Mechanisms, measurement and clinical implications in humans. Gut 2019, 68, 1516–1526. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.D. Bacterial translocation from the gastrointestinal tract. Mech. Pathog. Enteric Dis. 2 1999, 473, 11–30. [Google Scholar]
- Sommansson, A.; Saudi, W.S.W.; Nylander, O.; Sjöblom, M. Melatonin inhibits alcohol-induced increases in duodenal mucosal permeability in rats in vivo. Am. J. Physiol.-Gastrointest. Liver Physiol. 2013, 305, G95–G105. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren, D.; Roos, C.; Lundqvist, A.; Tannergren, C.; Sjöblom, M.; Sjögren, E.; Lennernäs, H. Time-dependent effects on small intestinal transport by absorption-modifying excipients. Eur. J. Pharm. Biopharm. 2018, 132, 19–28. [Google Scholar] [CrossRef]
- Rubbens, J.; Brouwers, J.; Wolfs, K.; Adams, E.; Tack, J.; Augustijns, P. Ethanol concentrations in the human gastrointestinal tract after intake of alcoholic beverages. Eur. J. Pharm. Sci. 2016, 86, 91–95. [Google Scholar] [CrossRef]
- Dahlgren, D.; Roos, C.; Lundqvist, A.; Langguth, P.; Tannergren, C.; Sjöblom, M.; Sjögren, E.; Lennernas, H. Preclinical effect of absorption modifying excipients on rat intestinal transport of five model compounds and the intestinal barrier marker 51Cr-EDTA. Mol. Pharm. 2017, 14, 4243–4251. [Google Scholar] [CrossRef]
- Blikslager, A.T.; Moeser, A.J.; Gookin, J.L.; Jones, S.L.; Odle, J. Restoration of barrier function in injured intestinal mucosa. Physiol. Rev. 2007, 87, 545–564. [Google Scholar] [CrossRef]
- Peters, K.; Dahlgren, D.; Lennernäs, H.; Sjöblom, M. Melatonin-activated receptor signaling pathways mediate protective effects on surfactant-induced increase in jejunal mucosal permeability in rats. Int. J. Mol. Sci. 2021, 22, 10762. [Google Scholar] [CrossRef]
- Thomsen, M.; Vitetta, L. Adjunctive treatments for the prevention of chemotherapy-and radiotherapy-induced mucositis. Integr. Cancer Ther. 2018, 17, 1027–1047. [Google Scholar] [CrossRef] [Green Version]
- Billeschou, A.; Hunt, J.; Kissow, H. Important endpoints and proliferative markers to assess small intestinal injury and adaptation using a mouse model of chemotherapy-induced mucositis. JoVE J. Vis. Exp. 2019, e59236. [Google Scholar] [CrossRef]
- Wardill, H.R.; Bowen, J.M.; Al-Dasooqi, N.; Sultani, M.; Bateman, E.; Stansborough, R.; Shirren, J.; Gibson, R.J. Irinotecan disrupts tight junction proteins within the gut: Implications for chemotherapy-induced gut toxicity. Cancer Biol. Ther. 2014, 15, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Menzies, I.; Pounder, R.; Heyer, S.; Laker, M.; Bull, J.; Wheeler, P.; Creamer, B. Abnormal intestinal permeability to sugars in villous atrophy. Lancet 1979, 314, 1107–1109. [Google Scholar] [CrossRef]
- Fihn, B.M.; Sjöqvist, A.; Jodal, M. Permeability of the rat small intestinal epithelium along the villus-crypt axis: Effects of glucose transport. Gastroenterology 2000, 119, 1029–1036. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren, D.; Cano-Cebrián, M.-J.; Olander, T.; Hedeland, M.; Sjöblom, M.; Lennernas, H. Regional intestinal drug permeability and effects of permeation enhancers in rat. Pharmaceutics 2020, 12, 242. [Google Scholar] [CrossRef] [Green Version]
- Dahlgren, D.; Lennernäs, H. Intestinal permeability and drug absorption: Predictive experimental, computational and in vivo approaches. Pharmaceutics 2019, 11, 411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlgren, D.; Cano-Cebrián, M.-J.; Hellström, P.M.; Wanders, A.; Sjöblom, M.; Lennernäs, H. Prevention of rat intestinal injury with a drug combination of melatonin and misoprostol. Int. J. Mol. Sci. 2020, 21, 6771. [Google Scholar] [CrossRef] [PubMed]
- Sedin, J.; Dahlgren, D.; Sjöblom, M.; Nylander, O. The Impact of alpha-adrenoceptors in the regulation of the hypotonicity-induced increase in duodenal mucosal permeability in vivo. Pharmaceutics 2021, 13, 2096. [Google Scholar] [CrossRef]
- Sangild, P.T.; Shen, R.L.; Pontoppidan, P.; Rathe, M. Animal models of chemotherapy-induced mucositis: Translational relevance and challenges. Am. J. Physiol.-Gastrointest. Liver Physiol. 2018, 314, G231–G246. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarek, A.; Brinkman, B.M.; Heyndrickx, L.; Vandenabeele, P.; Krysko, D.V. Severity of doxorubicin-induced small intestinal mucositis is regulated by the TLR-2 and TLR-9 pathways. J. Pathol. 2012, 226, 598–608. [Google Scholar] [CrossRef]
- Capaldo, C.T.; Nusrat, A. Cytokine regulation of tight junctions. Biochim. Biophys. Acta (BBA)-Biomembr. 2009, 1788, 864–871. [Google Scholar] [CrossRef] [Green Version]
- Melo, M.L.P.; Brito, G.A.; Soares, R.C.; Carvalho, S.B.; Silva, J.V.; Soares, P.M.; Vale, M.L.; Souza, M.H.; Cunha, F.Q.; Ribeiro, R.A. Role of cytokines (TNF-α, IL-1β and KC) in the pathogenesis of CPT-11-induced intestinal mucositis in mice: Effect of pentoxifylline and thalidomide. Cancer Chemother. Pharmacol. 2008, 61, 775–784. [Google Scholar] [CrossRef]
- Hamouda, N.; Sano, T.; Oikawa, Y.; Ozaki, T.; Shimakawa, M.; Matsumoto, K.; Amagase, K.; Higuchi, K.; Kato, S. Apoptosis, dysbiosis and expression of inflammatory cytokines are sequential events in the development of 5-fluorouracil-induced intestinal mucositis in mice. Basic Clin. Pharmacol. Toxicol. 2017, 121, 159–168. [Google Scholar] [CrossRef] [Green Version]
- Beukema, M.; Jermendi, É.; Koster, T.; Kitaguchi, K.; de Haan, B.J.; van den Berg, M.A.; Faas, M.M.; Schols, H.A.; de Vos, P. Attenuation of doxorubicin-induced small intestinal mucositis by pectins is dependent on pectin’s methyl-ester number and distribution. Mol. Nutr. Food Res. 2021, 65, 2100222. [Google Scholar] [CrossRef]
- Ferreira, T.M.; Leonel, A.J.; Melo, M.A.; Santos, R.R.; Cara, D.C.; Cardoso, V.N.; Correia, M.I.; Alvarez-Leite, J.I. Oral supplementation of butyrate reduces mucositis and intestinal permeability associated with 5-fluorouracil administration. Lipids 2012, 47, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Melichar, B.; Zezulová, M. The significance of altered gastrointestinal permeability in cancer patients. Curr. Opin. Supportive Palliat. Care 2011, 5, 47–54. [Google Scholar] [CrossRef]
- Stein, A.; Voigt, W.; Jordan, K. Chemotherapy-induced diarrhea: Pathophysiology, frequency and guideline-based management. Ther. Adv. Med. Oncol. 2010, 2, 51–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odenwald, M.A.; Turner, J.R. The intestinal epithelial barrier: A therapeutic target? Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Muehler, A.; Slizgi, J.R.; Kohlhof, H.; Groeppel, M.; Peelen, E.; Vitt, D. Clinical relevance of intestinal barrier dysfunction in common gastrointestinal diseases. World J. Gastrointest. Pathophysiol. 2020, 11, 114. [Google Scholar] [CrossRef]
- Sommansson, A.; Saudi, W.S.W.; Nylander, O.; Sjöblom, M. Effects of melatonin in ethanol-induced increases in duodenal mucosal permeability, motility and bicarbonate secretion in rats. Proc. Acta Physiol. 2015, 214, 2–3. [Google Scholar]
- Pihl, L.; Wilander, E.; Nylander, O. Comparative study of the effect of luminal hypotonicity on mucosal permeability in rat upper gastrointestinal tract. Acta Physiol. 2008, 193, 67–78. [Google Scholar] [CrossRef]
- Dahlgren, D.; Sjöblom, M.; Hedeland, M.; Lennernäs, H. The in vivo effect of transcellular permeation enhancers on the intestinal permeability of two peptide drugs enalaprilat and hexarelin. Pharmaceutics 2020, 12, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, R.J.; Bowen, J.M.; Inglis, M.R.; Cummins, A.G.; Keefe, D.M. Irinotecan causes severe small intestinal damage, as well as colonic damage, in the rat with implanted breast cancer. J. Gastroenterol. Hepatol. 2003, 18, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Blandizzi, C.; De Paolis, B.; Colucci, R.; Lazzeri, G.; Baschiera, F.; Del Tacca, M. Characterization of a novel mechanism accounting for the adverse cholinergic effects of the anticancer drug irinotecan. Br. J. Pharmacol. 2001, 132, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, R.J.; Bowen, J.M.; Alvarez, E.; Finnie, J.; Keefe, D.M. Establishment of a single-dose irinotecan model of gastrointestinal mucositis. Chemotherapy 2007, 53, 360–369. [Google Scholar] [CrossRef]
- Dahlgren, D.; Roos, C.; Peters, K.; Lundqvist, A.; Tannergren, C.; Sjögren, E.; Sjöblom, M.; Lennernäs, H. Evaluation of drug permeability calculation based on luminal disappearance and plasma appearance in the rat single-pass intestinal perfusion model. Eur. J. Pharm. Biopharm. 2019, 142, 31–37. [Google Scholar] [CrossRef]
- Cardiff, R.D.; Miller, C.H.; Munn, R.J. Manual hematoxylin and eosin staining of mouse tissue sections. Cold Spring Harb. Protoc. 2014, 6, 655–658. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intraperitoneal Dosing 72 h before SPIP | SPIP Exposure Period (15 min) |
|---|---|
| Saline, control (n = 18) | Buffer (n = 6) |
| SDS 5 mg/mL (n = 6) | |
| Ethanol 15% w/w (n = 6) | |
| Doxorubicin 10 mg/kg (n = 12) or Irinotecan 150 mg/kg (n = 12) or 5-Fluorouracil 200 mg/kg (n = 12) | SDS 5 mg/mL (n = 6) |
| Ethanol 15% w/w (n = 6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cano-Cebrián, M.-J.; Dahlgren, D.; Kullenberg, F.; Peters, K.; Olander, T.; Sjöblom, M.; Lennernäs, H. Chemotherapeutics Combined with Luminal Irritants: Effects on Small-Intestinal Mannitol Permeability and Villus Length in Rats. Int. J. Mol. Sci. 2022, 23, 1021. https://doi.org/10.3390/ijms23031021
Cano-Cebrián M-J, Dahlgren D, Kullenberg F, Peters K, Olander T, Sjöblom M, Lennernäs H. Chemotherapeutics Combined with Luminal Irritants: Effects on Small-Intestinal Mannitol Permeability and Villus Length in Rats. International Journal of Molecular Sciences. 2022; 23(3):1021. https://doi.org/10.3390/ijms23031021
Chicago/Turabian StyleCano-Cebrián, Maria-José, David Dahlgren, Fredrik Kullenberg, Karsten Peters, Tobias Olander, Markus Sjöblom, and Hans Lennernäs. 2022. "Chemotherapeutics Combined with Luminal Irritants: Effects on Small-Intestinal Mannitol Permeability and Villus Length in Rats" International Journal of Molecular Sciences 23, no. 3: 1021. https://doi.org/10.3390/ijms23031021