
Abstract
Introduction
Despite currently available treatments for adults with relapsed/refractory acute lymphoblastic leukemia (R/R ALL), survival outcomes remain poor, highlighting the need for new therapeutic strategies. This study estimates the cost-effectiveness of KTE-X19 to treat adults with R/R ALL from a US payer perspective.
Methods
The model had two components: a decision-tree, where pre-infusion costs for patients who ultimately did not receive KTE-X19 are accounted for, followed by a partitioned survival analysis, where all KTE-X19 infused patients would enter the three-state (pre-progression, progressed disease, death) model. Comparators included current standard of care treatments, i.e., blinatumomab (BLIN), inotuzumab ozogamicin (INO), and salvage chemotherapy (CHEMO). Both standard parametric and mixture cure models were used to model survival. Efficacy, safety, healthcare resource utilization, and health state utility inputs were derived from the ZUMA-3 trial (NCT02614066) and literature. Cost inputs were derived from literature or publicly available sources. Outcomes and costs were discounted 3% annually. Results of KTE-X19 versus comparators are reported as total and incremental life-years (LYs), quality-adjusted life-years (QALYs), costs, and resulting incremental cost-effectiveness ratio (ICER). Deterministic and probabilistic sensitivity analyses (PSA) and key scenario analyses were also performed.
Results
In the base case, incremental QALYs for KTE-X19 were 2.44, 3.26, and 4.61 versus BLIN, INO, and CHEMO, respectively. Incremental costs were $50,913, $251,532, and $432,027, respectively, resulting in ICERs of $20,843/QALY (versus BLIN), $77,271/QALY (versus INO), and $93,768/QALY (versus CHEMO). Deterministic sensitivity analysis results were most sensitive to subsequent allogeneic stem cell transplant rates and post-progression utilities. PSA found that KTE-X19 is 78.4%, 74.0%, and 75.4% likely to be cost-effective versus BLIN, INO, and CHEMO, respectively. Across most scenarios, at a willingness-to-pay (WTP) threshold of $150,000/QALY, KTE-X19 was cost-effective versus all treatments.
Conclusions
Compared to current options for adults with R/R ALL, KTE-X19 is cost-effective, driven primarily by improved survival.
Plain Language Summary
Several treatments for adults with relapsed/refractory B-cell precursor acute lymphoblastic leukemia (R/R B-ALL) have been approved in the past decade in the US, including blinatumomab (BLIN) and inotuzumab ozogamicin (INO). However, despite the high costs associated with these treatments, survival for patients remains poor. KTE-X19, an autologous anti-CD19 chimeric antigen receptor T-cell (CAR-T) therapy, approved by the Food and Drug Administration in October 2021, has potential to improve survival, but its economic value has not yet been determined. This model comprehensively evaluated the long-term clinical and economic value of KTE-X19 versus current treatments, including BLIN, INO, and salvage chemotherapy (CHEMO). Inputs were derived from key clinical trials, the literature, and other publicly available sources. The model used the perspective of a US third party payer over a patient lifetime. Compared to BLIN, INO and CHEMO, KTE-X19 resulted in improved quality of life as measured with incremental quality-adjusted life years (QALYs) of 2.44 (vs BLIN), 3.26 (vs INO), and 4.61 (vs CHEMO). Treatment with KTE-X19 had incremental costs of $50,913 (vs BLIN), $251,532 (vs INO), and $432,027 (vs CHEMO). KTE-X19 was found to provide good value for money based on incremental cost-effectiveness ratios of $20,843/QALY (vs BLIN), $77,271/QALY (vs INO), and $93,768/QALY (vs CHEMO). These values are well below the commonly accepted thresholds to determine economic value. Results were also found to be robust across sensitivity and scenario analyses.
Similar content being viewed by others

Why carry out this study? |
Adult patients with relapsed/refractory acute lymphoblastic leukemia (R/R ALL) have poor outcomes despite the availability of current treatments |
This study evaluated the cost-effectiveness of KTE-X19, a newly approved autologous anti-CD19 chimeric antigen T-cell therapy, versus currently recommended treatments of blinatumomab, inotuzumab ozogamicin and salvage chemotherapy in the US |
What was learned from the study? |
Treatment with KTE-X19 resulted in incremental cost-effectiveness ratios of $20,843 per quality-adjusted life year (QALY) versus blinatumomab, $77,271 per QALY versus inotuzumab ozogamicin and $93,768 per QALY versus salvage chemotherapy |
Driven by improved survival outcomes, KTE-X19 is a cost-effective treatment option compared to currently available therapies for adult patients with R/R ALL |
Introduction
Acute lymphoblastic leukemia (ALL) is a heterogeneous group of lymphoid disorders from the clonal proliferation of immature B- or T-cell lymphocytes in the blood, bone marrow, and other organs. In the US, ALL accounts for approximately 10% of all leukemias [1], and relapsed/refractory (R/R) ALL has an estimated incidence of < 1 in 100,000 individuals, with a prevalence of ~ 6 cases per 100,000 individuals [2]. Adult patients account for 47% of all ALL cases [3], and of them 75% were B-cell ALL [1].
Improvements in the risk-directed therapy of ALL consider factors such as age and minimal residual disease, among others. Adult R/R ALL carries a particularly poor prognosis, with median overall survival after relapse of approximately 7–8 months [4, 5]. Even with intensive salvage chemotherapy (CHEMO) followed by allogeneic stem cell transplantation (allo-SCT), cure rates among adults with R/R ALL are < 10% [6]. This may be due to advanced age, multiple comorbidities, higher-risk disease features, and heavy pre-treatment [7, 8]. In addition to poor clinical outcomes, R/R ALL is also associated with a substantial economic burden [9,10,11], attributed to disease progression and management of adverse events from available treatments [10, 12]. Multiple treatment options are currently available for adults with R/R-ALL in the US including those used as a bridge to allo-SCT (blinatumomab [BLIN], inotuzumab ozogamicin [INO]), other CAR-Ts (tisagenlecleucel for patients < 26 years of age and with R/R B-cell ALL disease in second or later relapse), and CHEMO. However, despite the availability of these treatments, survival outcomes among R/R ALL patients remain poor [4, 5].
KTE-X19 (brexucabtagene autoleucel) is an autologous anti-CD19 chimeric antigen receptor T-cell (CAR-T) therapy for the treatment of adult patients with R/R B-precursor ALL (B-ALL) and was approved by the Food and Drug Administration in 2021 [13]. KTE-X19 has shown promising efficacy in the phase 2 ZUMA-3 trial with 71% (95% CI 57–82; P < 0.0001) of treated patients in complete remission (CR) or complete remission with incomplete hematologic recovery (CRi), at a median follow-up of 16.4 months [14]. Median (95% confidence interval [CI]) duration of remission, relapse-free survival, and overall survival (OS) were 12.8 months (8.7–not estimable [NE]), 11.6 months (2.7–15.5), and 18.2 months (15.9–NE), respectively [13, 14]. To date, there have been no cost-effectiveness analyses of KTE-X19 in this setting. Given the high unmet need and significant economic burden of disease in patients with R/R B-ALL, a cost-effectiveness analysis of KTE-X19 versus currently available treatment options was undertaken to inform the allocation of limited healthcare resources.
Methods
Model Overview
An economic model was developed in Microsoft Excel® to evaluate the cost-effectiveness of KTE-X19 versus current treatment options for adult patients (≥ 18 years) with R/R B-ALL. The model structure included a decision tree prior to entry into a partitioned survival analysis. Treatment options were informed by current National Comprehensive Cancer Network (NCCN) guidelines for adult R/R ALL and include BLIN, INO, and CHEMO [15]. The analysis is from the perspective of a third-party US payer. Patients enter the model at a median age of 40 years (corresponding to the ZUMA-3 trial) and are followed for a lifetime time horizon of 59 years (until patients are 99 years of age). A cycle length of 1 week was used; costs and effects were discounted at 3% annually [16]. The model was developed in accordance with International Society for Pharmacoeconomics and Outcomes Research (ISPOR) guidelines [17]. This article is based in part on a previously conducted study and does not contain any new studies with human participation performed by any of the authors.
Model Structure
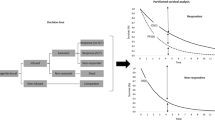
The model has two components: a decision tree component followed by a partitioned survival component (Fig. 1). The decision tree is included only for the KTE-X19 arm in order to account for the costs of pre-treatment for patients who may be assigned for treatment with KTE-X19 but ultimately did not receive the infusion because of adverse events, death, or other reasons (e.g., manufacturing issues, disease progression); this approach is consistent with other CAR T models [18]. Patients who did not receive KTE-X19 but survived the pre-infusion period were assumed to incur costs and experience survival of comparator therapies. Patients who did not receive KTE-X19 because of adverse events (AEs) are assumed to receive chemotherapy; the remaining non-infused patients are equally distributed across the comparator therapies in the model. All patients then enter the three-state partitioned survival in the pre-progression survival (PPS) state. Those who experience an event move to the progressed disease (PD) state, where the deteriorating quality of life of patients following disease progression prior to death is captured; patients may also receive subsequent treatment in this state. Death is an absorbing state, and patients can transition to it from any health state.

Model structure
Inputs
Patient Population
Baseline patient characteristics used in the economic model align with the modified intent-to-treat (mITT) population of the ZUMA-3 trial with a mean age of 42.1 years (n = 55), a mean body surface area of 1.95 m2, and 60.0% male patients.
Survival
Given the need to extrapolate beyond the follow-up period in both KTE-X19 and comparator arms, models were fit to estimate long-term survival for KTE-X19 and the comparator arms. Pseudo-individual patient data (IPD) based on available Kaplan-Meier (KM) plots and event information were generated using the algorithm described by Guyot et al. [19]. While standard parametric fitted curves (exponential, Weibull, log-logistic, lognormal, Gompertz, generalized gamma) were considered for model fit, to accurately reflect the clinical mechanisms of long-term remission, mixture cure models (MCMs) were also considered, using the flexsurvcure package in R [20]. MCMs assume that the observed survival in the trial population represents a blend of patients who are “cured” and “not cured,” perceived as a plateau in a KM curve, and allow for a change in the hazards of death over time [21]. Survival models were compared and assessed based on the following goodness-of-fit criteria: lowest Akaike information criteria (AIC) and Bayesian information criteria (BIC), where models with a difference in AIC and BIC of < 5 units are assumed to be of equal statistical fit; visual inspection of the fitted models overlaid on the KM curves; and clinical plausibility of long-term extrapolations beyond the trial period. Due to a lack of published long-term R/R ALL survival data in the US, in the base case, patients who were progression-free at 2 years were assumed to have achieved long-term remission and followed general US background mortality [22] with quality of life similar to the US general population. Additional scenario analyses on different excess mortality ratios were also examined.
KTE-X19
IPDs from the phase 2 ZUMA-3 trial were used to extrapolate survival for KTE-X19 [14]. The mITT population of the ZUMA-3 trial was used to determine survival of those who received a KTE-X19 infusion; for patients who were assigned to receive KTE-X19 in the decision tree but did not, survival was based on the assigned comparator arm. The ZUMA-3 trial measured relapse-free survival (RFS), defined as the time from KTE-X19 infusion to the date of disease relapse or death from any cause; patients who did not reach CR or CRi as of the data cutoff date were evaluated as having an RFS event at day 0. For the purpose of this analysis, RFS was used to inform survival in the PPS state. For RFS, MCM curves failed to capture the cure fraction for patients with long-term remission as observed in the KM curve (due to the low number of patients in the mITT population); therefore, a parametric model with a 2-year cure assumption was used, where patients without progression at 2 years are assumed to achieve long-term remission and subsequently follow the US general population mortality rate, in line with the cost-effectiveness analysis of BLIN vs INO [23]. Based on the AIC/BIC fit, the generalized gamma model was considered in the base case with a cure assumed at 2 years. For OS, however, standard parametric survival curves failed to capture the change in the hazard of death associated with the observed plateau for OS; therefore, an exponential MCM was used to adequately capture the cure fraction (estimated at 29.6%) (Supplementary Material Fig. S1 and Table S1).
Blinatumomab
To inform survival in patients receiving BLIN, the TOWER trial in Philadelphia-negative (Ph-) B-ALL patients was used [5]. While the TOWER population does not include Philadelphia-positive (Ph +) B-ALL patients, results were similar to the ALCANTARA trail in Ph + B-ALL patients [24]. For EFS, the AIC/BIC values were similar for both standard parametric curves and MCMs. However, based on the visual fit, the Weibull MCM was chosen for the EFS base case analysis, resulting in a 7.67% cure fraction; this is consistent with the plateau observed in the TOWER trial [5]. The OS base case analysis curve was selected based on the visual fit, with the Weibull MCM resulting in a 19.8% cure fraction; this cure fraction is consistent with the plateau observed in both the TOWER trial and clinical practice [25] (Supplementary Material Fig. S2, Table S1).
Inotuzumab Ozogamicin
Data to inform INO were taken from the long-term survival follow-up INO-VATE trial of patients with R/R B-ALL [4]. For EFS, based on the lowest AIC/BIC, the lognormal MCM, with a 13.74% cure fraction, was chosen for the base case analysis; this is consistent with the plateau observed in INO-VATE [4]. For the OS extrapolation, the loglogistic MCM was chosen for the base case analysis, based on the lowest AIC/BIC and visual fit to the KM data, resulting in a 13.1% cure fraction. The selected base case curves and goodness-of-fit are presented in Figure S3 and Table S1 (Supplementary Material), respectively.
Chemotherapy
Survival data to inform the CHEMO comparator arm were also taken from the INO-VATE trial [4] given its longer duration of study follow-up in the trial. Based on the lowest AIC/BIC, the lognormal MCM was chosen for the base case EFS analysis, resulting in a 3.89% cure fraction. For the OS base case analysis, based on the lowest AIC/BIC, the exponential MCM was chosen, resulting in a 7.0% cure fraction. For both EFS and OS, the models are consistent with both the trends observed in the INO-VATE trial [4] as well as with real-world evidence for R/R ALL chemo-treated patient survival [26]. Base case survival curves and goodness-of-fit for CHEMO are presented in Fig. S4 and Table S1, respectively (Supplementary Material).
Scenario Analysis with Synthetic Control Arm
A scenario analysis was performed to compare outcomes of patients treated with KTE-X19 to IPD sampled from historical clinical trials of patients who had not previously failed blinatumomab. A post hoc analysis of the SCHOLAR-3 study was done using a synthetic control matching patients from ZUMA-3 (irrespective of pre-treatment with BLIN or INO) to BLIN- or INO-naïve patients from historical clinical trials (synthetic control arm 3 [SCA-3]) [27]. As patients in SCA-3 could have received either BLIN (92.5%) or standard of care chemotherapy (7.5%), the study population was further restricted to only reflect patients who received BLIN in the SCA-3 arm. Cohorts were well balanced, with the standardized mean difference across all characteristics below the 0.25 threshold (Table S2). For the KTE-X19 arm, parametric survival models were applied for a period of 2 years followed by the US general population mortality rate. A parametric lognormal model was used for both EFS and OS because of superior visual fit of the KM data. For the SCA-3 cohort analysis, for EFS, a loglogistic parametric survival model was applied for a period of 2 years, followed by the US general population mortality rate. For the extrapolation of OS, a parametric lognormal function was chosen; the selected EFS and OS curves from the SCA-3 scenario analyses and the selected EFS and OS curves for KTE-X19 and BLIN are shown in the Supplementary Material (Figures S6 and S7 with goodness-of-fit presented in Table S3).
Safety Inputs
Incidence of AEs were included based on the respective clinical trials (Table S4, Supplementary Material). Post-infusion grade 3 or 4 AEs occurring in ≥ 5% of the ZUMA-3 population were included for KTE-X19 [14]. For BLIN, grade ≥ 3 AEs occurring in ≥ 5% of the TOWER study population in the first cycle of therapy were included [28]. Serious AEs reported in ≥ 2% of the INO-VATE safety population were used for INO [4]. AE rates for CHEMO were pooled from the CHEMO arms of the INO-VATE [4] and TOWER trials [28]. These rates were varied in the sensitivity analyses.
Cost and Resource Use
Costs considered in the model included all drug acquisition and administration costs (including allo-SCT costs); subsequent treatment costs; monitoring costs for both the PPS and PD health states; terminal care costs; and costs associated with managing adverse events (summarized in Table 1 with additional detail in the Supplementary Material). Vial sharing was not considered in the calculation of drug acquisition costs in the base case; the number of vials per dose was rounded up to the nearest vial. All costs were sourced in 2021 are reported in 2021 US dollars and were inflated using the US Bureau of Labor Statistics Consumer Price Index for medical care services [29].
KTE-X19 Costs
KTE-X19 is associated with costs prior to receiving an infusion. Given that all patients scheduled to receive KTE-X19 incur pre-treatment costs, but not all patients go on to receive the infusion, a correcting factor was applied to the mITT population to account for all pre-treatment costs in the population who received the infusion. Pre-treatment costs were applied in the first cycle of the model for KTE-X19 patients. It was assumed all KTE-X19 patients would receive leukapheresis. Based on the ZUMA-3 trial, all patients received a single, 3-day round of conditioning chemotherapy: it was assumed that 65% of patients would receive this in the inpatient setting and 35% would receive it in the outpatient setting [25]. Conditioning therapy prior to infusion was given as cyclophosphamide (900 mg/m2/day) for 1 day and fludarabine (25 mg/m2/day) for 3 days. Bridging therapy was included for all patients as a weighted average of the regimens observed in the ZUMA-3 trial; bridging therapy was assumed to be administered in the inpatient setting. It was assumed that KTE-X19 patients were hospitalized for an average of 23.67 days for the infusion, with an average of 4 days spent in the intensive care unit; this is in addition to pre-treatment costs [30]. The cost of a single, one-time infusion of KTE-X19 was based on the list price of $399,000 [31]. Costs for patients who were scheduled to receive KTE-X19 but did not were accounted for as a weighted average of the comparator regimens described below.
Comparator Costs
BLIN was administered on inpatient basis for the first 9 days of cycle 1 and first 2 days of cycle 2 and via a pump for the remainder of cycle 1 and for cycles 2 +; the required bag change in the outpatient setting (every 2 days [23]) was included in the administration cost. INO dosing was based on the INO-VATE trial, with four vials administered per cycle, and three intravenous (IV) administrations per cycle to a maximum of six total cycles. CHEMO was costed as FLAG-IDA based on both the NCCN guidelines and its similar cost and efficacy to other regimens as fludarabine (30 mg/m2 for 5 consecutive days per 28-day cycle for up to four cycles); cytarabine (2 gm/m2 for 6 consecutive days per 28-day cycle for up to four cycles); filgrastim (0.005 mg/kg for 9 total days); and idarubicin (8 mg/m2 for 3 days per 28-day cycle). Maximum treatment duration for CHEMO was estimated to be 4 cycles, with a total of 11 inpatient days of administration per cycle. All patients who start each cycle of treatment are assumed to complete the cycle; total cycle costs were applied at entry to the PPS health state.
Subsequent Allo-SCT
The model assumed that in lieu of subsequent treatments, some patients may receive an allo-SCT. Allo-SCT costs were determined by multiplying the cost of an allo-SCT including 24 months of follow-up ($416,823[10, 23]) by the proportion of patients receiving an allo-SCT by treatment arm (Table 1).
Subsequent Treatment Costs
Following progression on treatment, patients could receive a subsequent treatment. Distribution of subsequent treatments was based on the ZUMA-3 trial. As patients were assumed not to be re-treated with their initial therapy, the distribution of subsequent treatments was re-weighted to remove re-treatment of their prior therapy. Patients who initially received CHEMO were assumed to receive the same composition of subsequent treatment as those who had received KTE-X19. Subsequent treatment costs were applied as a one-time weighted cost upon progression and include both drug acquisition and drug administration costs (Table 1).
Monitoring Costs
Monitoring and follow-up resource use for the PPS and PD state were applied at the same frequency across all comparators. These consisted of outpatient visits; relevant clinical tests and procedures were based on the submission of tisagenleclecel to the National Institute for Health and Care Excellence [25]. The frequency of resource use was validated by US clinical experts [32] (Table S7, Supplementary Material). No further monitoring and follow-up costs were included for patients who received an allo-SCT, as these were included in the cost of the allo-SCT. All unit costs were derived from the Centers for Medicare & Medicaid Services (CMS) Physician and Laboratory Fee Schedules [33, 34].
Terminal care
All patients transitioning to death incurred a one-time terminal care cost of $28,527 [23, 35].
Management of Adverse Events
Costs to manage treatment-related AEs were applied as a one-time cost in the first cycle of the model. AEs occurring during the infusion period for KTE-X19, including neurologic toxicity, were assumed to be managed during the inpatient admission. Cytokine release syndrome (CRS) is specific to treatment with both KTE-X19 and BLIN and was assumed to be managed with tocilizumab (8 mg/kg daily) [14], a conservative cost assumption compared to treatment with steroids. The total one-off AE costs applied per treatment regimen are summarized in Table 1; detailed unit costs for all AEs are provided in Table S8 (Supplementary Material).
Health State Utilities
Published utility values were available for KTE-X19 [14], BLIN [23], and CHEMO [23] (Table 1). In the absence of utility data to align with the modeled states for INO, values were assumed to be the same as BLIN[23]. For all treatment arms, patients who achieved long-term remission were assumed to have the same health utility value as the US general population [36]. Age-adjusted utility decrements related to the occurrence of AEs were applied using a one-time value in the first cycle of the model and were derived by multiplying the utility decrement by the duration of the AE (Table S9, Supplementary Material). In addition to AE utility decrements, treatment-related utility decrements were applied. For the pre-treatment/hospitalization period, a utility decrement of – 0.42 [37] was applied for patients receiving BLIN or CHEMO for durations of 21.0 and 9.2 days, respectively [25, 37]. For patients receiving an allo-SCT, an additional utility decrement of – 0.57 [37] for 1 year was applied to capture the impact of potential complications or AEs associated with allo-SCT.
Outcomes
Outcomes reported include life-years (LYs), quality-adjusted life-years (QALYs), and total costs. The incremental cost-effectiveness ratio (ICER) was calculated as the incremental cost divided by the incremental QALYs. All results are presented as discounted over a lifetime time horizon (59 years).
Sensitivity Analyses
Both univariate and probabilistic sensitivity analyses were conducted. Inputs were varied using the reported standard error (SE); in cases where the SE was not reported, it was assumed to be 20%. Results from univariate sensitivity analyses are presented in tornado diagrams where the ten most influential model parameters are outlined. The results of the probabilistic sensitivity analysis are plotted on a cost-effectiveness plane, where the incremental results versus a given comparator is plotted. Cost-effectiveness acceptability curves present the probability that each treatment is cost-effective at willingness to pay thresholds from $0 to $200,000/QALY.
Scenario Analyses
Scenario analyses examined the impact of model time horizon, discount rate, AE costs, excess mortality for patients with long-term remission via standardized mortality ratios (SMRs), and alternate utility / disutility values.
Results
Overall Population
Model estimated survival for PPS and OS for KTE-X19 and all comparators are presented in Table 2. Model estimated PPS at 5, 10, and 15 years was highest for treatment with KTE-X19; median PPS for treatment with KTE-X19 was 5.5 months. OS rates were also highest for treatment with KTE-X19; median OS for KTE-X19 as estimated by the model was 23.7 months.
Treatment costs (drug acquisition and administration), subsequent treatment costs, and allo-SCT costs are presented in Table 3. Drug acquisition and administration costs in the PPS state represented the largest proportion of costs.
Total LYs and QALYs were highest for KTE-X19; incremental gains were 2.83 LYs and 2.44 QALYs versus BLIN, 3.96 LYs, and 3.26 QALYs versus INO; and 5.58 LYs and 4.61 QALYs versus CHEMO (Table 4). Assuming a list price for KTE-X19 of $399,000, the discounted incremental costs of KTE-X19 versus BLIN, INO, and CHEMO were $50,913, $251,532, and $432,027, respectively. The ICERs for KTE-X19 versus BLIN, INO, and CHEMO were $20,843/QALY, $77,271/QALY, and $93,768/QALY, respectively.
Synthetic Control Arm Scenario Analysis
When comparing KTE-X19 to BLIN-naïve patients using the SCA-3 historical control dataset, OS outputs estimated by the model were 36.73%, 33.43%, and 30.94% at 5, 10, and 15 years for KTE-X19, respectively, and 18.52%, 18.17%, and 17.63% at 5, 10, and 15 years for BLIN, respectively. The main contributor to the total costs were drug acquisition costs (Table S10). Median OS was estimated to be 15.64 months for KTE-X19 and 7.82 months for BLIN. The ICER for KTE-X19 versus BLIN was $25,274/QALY (Table S11).
Sensitivity Analyses
Deterministic one-way sensitivity analysis results for KTE-X19 versus each of the base case analysis comparators are provided in Fig. 2, panels i, ii and iii. Overall, the key drivers of cost-effectiveness outcomes for KTE-X19 across comparators were related to the proportions of patients receiving allo-SCT and utility values. Other factors included the duration of bridging therapy (versus BLIN) and the number of inpatient days for treatment (CHEMO) (see Table 5).


One-way sensitivity analysis results: KTE-X19 versus comparators
The cost-effectiveness acceptability curve for KTE-X19 shows that at a WTP threshold of $150,000/QALY, KTE-X19 would be considered cost-effective in approximately 78.4%, 74.0%, and 75.4% of scenarios compared to BLIN, INO, and CHEMO.
Additional Scenario Analyses
KTE-X19 was cost-effective in nearly all scenarios versus BLIN, INO and CHEMO at a WTP of $150,000/QALY.
Discussion
Treatment of patients with R/R adult ALL remains a challenge; current treatments do not offer meaningful survival benefits. This study evaluated the cost-effectiveness of KTE-X19 using recent results from the ZUMA-3 clinical trial versus BLIN, INO, and salvage therapy in adults with R/R B-ALL. Overall, based on the observed survival benefit in the ZUMA-3 trial, the model estimated incremental gains of 2.44 QALYs, 3.26 QALYs, and 4.61 QALYs versus BLIN, INO, and CHEMO, respectively. Over a lifetime time horizon, KTE-X19 was cost-effective versus all comparators at a WTP threshold of $150,000/QALY. Furthermore, sensitivity analyses found that the model outcomes, across all comparators, were robust to changes in inputs and assumptions through the OWSA and the scenario analyses. These results suggest that, in addition to the estimated longer survival of patients with R/R adult ALL, treating patients with KTE-X19 in the R/R setting is cost-effective, representing an efficient use of healthcare resources.
Treatment with KTE-X19 offers a new promising option for patients with R/R adult B-ALL. While the upfront cost of CAR T-cell therapy is higher than that of current cancer drugs, this novel form of cancer immunotherapy provides increased efficacy driven by their survival advantages. Based on data from the Cost-Effectiveness Analysis Registry of the Tufts Medical Center and the Institute for Clinical and Economic Review’s analysis of CAR-T therapies, CAR-Ts provide significantly greater effectiveness than prior pharmaceutical innovations [38], providing incremental gains of 5.03 QALYs above the average pharmaceutical intervention, addressing a large unmet in patients. Despite their high up-front costs, the cost-effectiveness of CAR-T therapies has previously been evaluated in other indications and therapy areas. In pediatric R/R B-cell ALL, CAR-T therapy, compared to standard of care, was found to result in an ICER of $64,600/QALY and was cost-effective in 94.8% of iterations at a WTP of $100,000/QALY[39]. Simons et al. found that KTE-X19 was cost-effective for adult patients with R/R mantle cell lymphoma in the US, with an ICER of $31,985/QALY versus standard of care [40].
The findings in this analysis should be interpreted in the context of some key limitations. Data informing the effectiveness across the recommended treatments for R/R B-ALL in the base case were based on a systematic literature review of R/R ALL publication as of November 2020; thus, longer term follow-up for comparators was not incorporated in the extrapolation. Furthermore, the indirect comparisons with the TOWER and INO-VATE trial were based on naïve comparisons without further risk profile adjustment. However, when considering the SCHOLAR-3 analysis of matched patients versus BLIN, similar results were observed. Of note, CHEMO regimens across clinical practices may vary; thus, the cost and survival associated with CHEMO treatment were varied to reflect alternate regimens; results were similar to the base case analysis. It should also be noted that monitoring and follow-up resource use along with adverse event management may differ between real-world clinical practices. While not all possible differences may have been captured in the scenario analyses, these were not key drivers in costs. While it is a reasonable assumption that no patients achieve remission following relapse, it is clinically plausible that a small proportion of patients in the PD state may do so with subsequent line of treatments for up to 5 years after relapse. This assumption, however, was not considered as previous modeling studies found no significant impact on model results when including this scenario [25]. Survival in the PPS state was informed by the respective clinical trials. While the ZUMA-3 trial reported RFS, and not EFS, this was considered conservative as RFS measures disease progression (i.e., those not achieving CR or CRi) or death from any cause from the date of infusion versus EFS, which includes CR with partial recovery in addition to CR/CRi and is measured from randomization. Given the limited clinical experience with CAR-T therapies for the treatment of adults with R/R-ALL, there is no clear consensus as to how allo-SCT should be used following CAR-T therapy in clinical practice. As such, with the limited data available and the small number of patients receiving an allo-SCT after KTE-X19 in the ZUMA-3 trial, it was not possible to stratify survival by receipt of allo-SCT. However, while the survival impact of allo-SCT is not considered, the impact of allo-SCT in terms of quality of life and costs was accounted for in the model and proportion receiving allo-SCT were varied in sensitivity analyses. Furthermore, this analysis did not consider tisagenlecleucel as a comparator. While tisagenlecleucel is recommended for those < 26 years of age, there was limited overlap in pages aged 18–25 years between clinical trials for KTE-X19 and tisagenlecleucel [41]; the inclusion of tisagenlecleucel would have thus resulted in a small sample size and high uncertainty in model outcomes. Patients who did not receive KTE-X19 due to AEs were assumed to receive chemotherapy; while it is possible that patients would have performed better on BLIN or INO, this assumption has minimal impact on the model results. Finally, it should be noted that, as with many cost-effectiveness analyses, the real-world outcomes and healthcare resource use associated with each of these treatments is likely to vary from those observed in the clinical trials and across geographies and health systems.
Conclusions
This study found that KTE-X19 results in improved health outcomes with acceptable incremental costs compared to BLIN, INO, or CHEMO. KTE-X19 may be considered a cost-effective therapy for adult R/R B-ALL patients.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30.
Spoorendonk J, Feng C, Shah D, et al. PCN183 global incidence, prevalence, and survival in relapsed/refractory (R/R) adult acute lymphoblastic leukemia (aALL): a systematic literature review (SLR). Value Health. 2020;23:S455.
National Cancer Institute. SEER Cancer Statistics Review (CSR) 1975–2018. In: Howlader N, Noone A, Krapcho M, et al., editors. SEER Cancer Statistics Review (CSR) 1975-2018. Bethesda, 2021.
Kantarjian HM, DeAngelo DJ, Stelljes M, et al. Inotuzumab ozogamicin versus standard of care in relapsed or refractory acute lymphoblastic leukemia: Final report and long-term survival follow-up from the randomized, phase 3 INO-VATE study. Cancer. 2019;125(14):2474–87.
Kantarjian H, Stein A, Gökbuget N, et al. Blinatumomab versus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med. 2017;376(9):836–47.
Samra B, Jabbour E, Ravandi F, et al. Evolving therapy of adult acute lymphoblastic leukemia: state-of-the-art treatment and future directions. J Hematol Oncol. 2020;13(1):70.
Rowe JM. Prognostic factors in adult acute lymphoblastic leukaemia. Br J Haematol. 2010;150(4):389–405.
Sarfati D, Koczwara B, Jackson C. The impact of comorbidity on cancer and its treatment. CA Cancer J Clin. 2016;66(4):337–50.
Zhu F, Wei G, Zhang M, et al. Factors associated with costs in chimeric antigen receptor T-cell therapy for patients with relapsed/refractory B-cell malignancies. Cell Transplant. 2020;29:963689720919434.
Zhang X, Song X, Lopez-Gonzalez L, et al. Economic burden associated with adverse events of special interest in patients with relapsed Philadelphia chromosome-negative B-cell acute lymphoblastic leukemia in the United States. Expert Rev Pharmacoecon Outcomes Res. 2018;18(5):573–80.
Cool C, Feng C, Wade S, et al. Healthcare resource utilization and costs in adult patients with relapsed or refractory acute lymphoblastic leukemia using real-world data from the United States. In: Pan Pacific Lymphoma Conference; Big Island, Hawaii 2021.
Zhang X, Song X, Lopez-Gonzalez L, et al. Economic burden of veno-occlusive disease in patients with B-cell acute lymphoblastic leukemia in the United States. Clin Ther. 2018;40(10):1711–1719.e1.
Food and Drug Administration. TECARTUS: Highlights of prescribing information. 2021. https://www.fda.gov/media/140409/download.
Shah BD, Ghobadi A, Oluwole OO, et al. KTE-X19 for relapsed or refractory adult B-cell acute lymphoblastic leukaemia: phase 2 results of the single-arm, open-label, multicentre ZUMA-3 study. The Lancet. 2021;398(10299):491–502.
Brown PA, Shah B, Advani A, et al. Acute lymphoblastic leukemia, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2021;19(9):1079–109.
Gold MRSJ, Russell LB, Weinstein MC. Cost effectiveness in health and medicine. New York: Oxford University Press; 1996.
Caro JJ, Briggs AH, Siebert U, et al. Modeling good research practices–overview: a report of the ISPOR-SMDM Modeling Good Research Practices Task Force-1. Med Decis Making. 2012;32(5):667–77.
Institute for Clinical and Econoc Review. Chimeric Antigen Receptor T-Cell Therapy for B-Cell Cancers: Effectiveness and Value. Final Evidence Report. In: California Technology Assessment Forum, editor. 2018. https://collections.nlm.nih.gov/catalog/nlm:nlmuid-101744954-pdf
Guyot P, Ades AE, Ouwens MJNM, et al. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9.
flexsurv. Flexible parametric survival and multi-state models. 2021. https://cran.rproject.org/web/packages/flexsurv/flexsurv.pdf
Lambert PC, Thompson JR, Weston CL, et al. Estimating and modeling the cure fraction in population-based cancer survival analysis. Biostatistics. 2007;8(3):576–94.
Social Security Administration. Actuarial Life Table 2017. https://www.ssa.gov/OACT/STATS/table4c6_2017.html. Accessed 22 Apr 2021.
Delea TE, Zhang X, Amdahl J, et al. Cost effectiveness of blinatumomab versus inotuzumab ozogamicin in adult patients with relapsed or refractory B-cell precursor acute lymphoblastic leukemia in the United States. Pharmacoeconomics. 2019;37(9):1177–93.
Pulte ED, Vallejo J, Przepiorka D, et al. FDA supplemental approval: blinatumomab for treatment of relapsed and refractory precursor B-cell acute lymphoblastic leukemia. Oncologist. 2018;23(11):1366–71.
NICE-National Institute for Health and Care Excellence. Tisagenlecleucel for treating relapsed or refractory B-cell acute lymphoblastic leukaemia in people aged up to 25 years. [TA554]. 2018. https://www.nice.org.uk/guidance/ta554/resources/tisagenlecleucel-for-treating-relapsed-or-refractory-bcell-acutelymphoblastic-leukaemia-in-people-aged-up-to-25-years-pdf-82607021872837.
Gökbuget N, Dombret H, Ribera J-M, et al. International reference analysis of outcomes in adults with B-precursor Ph-negative relapsed/refractory acute lymphoblastic leukemia. Haematologica. 2016;101(12):1524–33.
Shah B, Faghmous I, Whitmore J, et al. The comparison of KTE-X19 to current standards of care: a pre-specified synthetic control study utilizing individual patient level data from historical clinical trials (SCHOLAR-3). In: American Society of Hematology: Annual Meeting & Exposition; December 11–14, 2021; Atlanta, Georgia2021.
Stein A, Franklin JL, Chia VM, et al. Benefit-risk assessment of blinatumomab in the treatment of relapsed/refractory B-cell precursor acute lymphoblastic leukemia. Drug Saf. 2019;42(5):587–601.
US Bureau of Labor Statistics. Consumer price index for medical care services. 2021. https://www.bls.gov/cpi/.
KITE. A study evaluating brexucabtagene autoleucel (KTE-X19) in adult subjects with relapsed/refractory B-precursor acute lymphoblastic leukemia (ZUMA-3). In: Data on file, editor.
IBM Micromedex RED BOOK. 2021. https://www.ibm.com/products/micromedex-red-book. Accessed 22 Apr 2021.
KITE. Expert clinical opinion, data on file.
CMS Laboratory Fee Schedule. 2021. Available from: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ClinicalLabFeeSched
CMS Physician Fee Schedule. 2021. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched. Accessed 22 Apr 2021.
Chastek B, Harley C, Kallich J, et al. Health care costs for patients with cancer at the end of life. J Oncol Pract. 2012;8(6):75s–80s.
Sullivan PW, Slejko JF, Sculpher MJ, et al. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making. 2011;31(6):800–4.
Sung L, Buckstein R, Doyle JJ, et al. Treatment options for patients with acute myeloid leukemia with a matched sibling donor: a decision analysis. Cancer. 2003;97(3):592–600.
Baumgardner JR, Brauer MS, Zhang J, et al. CAR-T therapy and historical trends in effectiveness and cost–effectiveness of oncology treatments. J Comp Effect Res. 2020;9(5):327–40.
Sarkar RR, Gloude NJ, Schiff D, et al. Cost-effectiveness of chimeric antigen receptor T-Cell therapy in pediatric relapsed/refractory B-cell acute lymphoblastic leukemia. J Natl Cancer Inst. 2019;111(7):719–26.
Simons CL, Malone D, Wang M, et al. Cost-effectiveness for KTE-X19 CAR T therapy for adult patients with relapsed/refractory mantle cell lymphoma in the United States. J Med Econ. 2021;24(1):421–31.
Maude SL, Laetsch TW, Buechner J, et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med. 2018;378(5):439–48.
Shah B, Smith N, Raad A, et al. ALL-190: cost-effectiveness of KTE-X19 for adult patients with relapsed/refractory B-cell acute lymphoblastic leukemia (R/R B-ALL) in the United States. Clin Lymphoma Myeloma Leuk. 2021;21:S272–3.
American Red Cross. Reimbursement Update. Available from: https://www.redcrossblood.org/content/dam/redcrossblood/forms-and-certificates/hospitalreimbursementupdate_2019.pdf.
Acknowledgements
Funding
This work was funded by Kite Pharmaceuticals, A Gilead Company. Kite Pharmaceuticals funded the Rapid Service and Open Access Fees for this study.
Medical Writing and Editorial Assistance
We acknowledge the editorial assistance in the preparation of this manuscript provided by Dr. Lianne Barnieh from Maple Health Group, LLC. We also thank Dr. Christine Fu and Dr. Tsveta Hadjivassileva of Medical Affairs from Kite, A Gilead Company for important contributions to the manuscript. We also thank Dr. Angie Raad, PhD, for assistance in the development of the analysis presented in this manuscript.
Author Contributions
All authors contributed to the study conception and design of the study. Data analyses were performed by Nathaniel J Smith and Sushanth Jeyakumar. The first draft of the manuscript was written by Nathaniel J Smith and Sushanth Jeyakumar and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Prior Presentation
This preliminary finding of this study was previously presented at the Society for Hematologic Oncology 2021 Annual Meeting [42].
Disclosures
Bijal D. Shah has received consulting fees from Kite Pharmaceuticals, A Gilead Company. Nathaniel J. Smith PhD has received consulting fees from Kite Pharmaceuticals, A Gilead Company. Chaoling Feng is an employee of Kite Pharmaceuticals, A Gilead Company. Sushanth Jeyakumar has received consulting fees from Kite Pharmaceuticals, A Gilead Company. Jean-Gabriel Castaigne is an employee of Kite Pharmaceuticals, A Gilead Company. Imi Faghmous is an employee of Kite Pharmaceuticals, A Gilead Company. Behzad Kharabi Masouleh is an employee of Kite Pharmaceuticals, A Gilead Company. Daniel C. Malone has received consulting fees from Kite Pharmaceuticals, A Gilead Company. Michael R. Bishop has received consulting fees from Kite Pharmaceuticals, A Gilead Company.
Compliance with Ethics Guidelines
This article is based in part on a previously conducted study and does not contain any new studies with human participation performed by any of the authors.
Data Availability
The data that support the findings from this study are available from the corresponding author, Nathaniel J. Smith, upon reasonable request.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Shah, B.D., Smith, N.J., Feng, C. et al. Cost-Effectiveness of KTE-X19 for Adults with Relapsed/Refractory B-Cell Acute Lymphoblastic Leukemia in the United States. Adv Ther 39, 3678–3695 (2022). https://doi.org/10.1007/s12325-022-02201-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-022-02201-6